Sleep and Circadian F.A.Q.
Some answers to commonly asked questions about sleep by Andrew Phillips
- What basics about sleep do I need to know before I read this?
- Does sleep loss cause weight gain?
- Is sleep deprivation lethal for humans?
- Are polyphasic sleep schedules effective?
- How much sleep must you lose to negatively affect immune function?
- Could we one day develop technologies or drugs to supplant the need for sleep?
- Why do we sleep lying down?
- Does sleeping position affect bone growth?
- What determines when we change positions during the night?
- Why is insomnia so common these days?
- Do biorhythms have any scientific basis?
- What is actually happening in the brain to make you sleepy the longer you are awake?
- What is the difference between sleeping for a certain period of time and lying in bed awake with your eyes closed?
- Is it possible to adapt to daytime sleeping?
- Do all animals sleep?
- Can falling asleep on my arm be dangerous?
- Why does inadequate sleep cause dark circles under the eyes?
- Why must eyes be closed to sleep?
- Are we meant to sleep in 8 hour blocks?
- What happens if I leave the lights on at night?
- Do dreams occur in real-time?
- Is dream analysis valid?
- What determines our dream content?
- How long does it take the brain to transition from sleep to wake?
- What is happening when I push through sleepiness?
- Why do fevers cause strange dreams?
- Do stressful dreams have the same effect on the body as stressful situations in real life?
- Does it matter which stage of sleep you wake from?
- Did people used to sleep earlier than they do today?
- Do some people just need less sleep?
- If you sleep without an alarm clock, do you sleep the exact amount of time you need?
- Is it better to get a tiny bit of sleep or to get no sleep at all?
- Why don’t we roll off our beds at night?
- Does lucid dreaming exist and is it different from regular REM sleep?
- Do babies dream?
- What causes sleep talking?
- Could humans live on a planet or a schedule with a period different from 24 hours?
- Do other animals dream?
- Why don’t bears lose muscle mass while hibernating?
- Why do you start to feel better in the morning after staying awake all night?
- Is sleep just a byproduct of the fact that Earth rotates?
- What is unihemispheric sleep?
- What is the difference between sleep and coma or unconsciousness or anesthesia?
- How can a sleep schedule be shifted earlier?
- Does taking melatonin actually work?
- Is jet lag largely unavoidable?
- Is it more useful to take a short nap, to help cope with a shift in sleeping pattern, or is it better to stay awake (or lie in bed, depending on what you're trying to do)?
- How does alcohol affect sleep?
- What is ''sleep'' in the eyes?
- How long does sleep debt build up for?
- Do people ever sneeze while asleep?
- Why do we prefer a dark environment for sleeping?
- Why does sleep loss cause headaches?
- Does sleep deprivation affect neurotransmitter levels in the brain?
- What basics do I need to know about sleep before I read this?
- Sleep is best defined in mammals as: a period of reduced activity, and often changed posture, reduced responsiveness to environmental stimuli, ability to rapidly return to wake if a strong enough stimulus is provided, rest that is homeostatically preserved (i.e. lost sleep results in a sleep debt and impaired functioning while awake), and well-defined changes in physiological signals, including brain activity changes associated with REM and NREM sleep.
Rapid Eye Movement (REM) Sleep: During this stage, brain activity looks similar to wake. However, you have very little muscle tone, and you are usually dreaming.
Non-REM (NREM) Sleep Stages 1-3: Stages 1-3 are in progressing order of depth. It is the hardest to wake someone during the deepest NREM sleep, and the brain activity includes progressively more large amplitude slow waves the deeper into NREM sleep. - Circadian rhythms are distinct from sleep, but fundamentally related. A circadian rhythm is any approximately 24 h rhythm that is endogenously generated by an organism. In other words, it is not just a response to environmental (exogenous) cues, though its phase can be reset by environmental cues, allowing it to remain synchronized to the light/dark cycle. Circadian rhythms can manifest in behavior (e.g., sleep/wake), physiological outputs (e.g., hormone release), biochemical processes, or gene expression.
- Virtually all species on this planet have evolved to live on a 24-h day. For this reason, we contain circadian clocks that time not only our activities and sleep, but also a million other things, including our hormone release, our metabolic cycles, our blood pressure rhythms, etc. Different species have adapted to be active during different parts of the day. Humans have evolved to be diurnal (day-active) and to get the large majority of our sleep during the night. We are not unique in this; several other primates also sleep in a relatively consolidated block during the night. Consequently, our body sends a very strong sleep signal during the night and a very strong wake signal during the day. For this reason, it is generally difficult to initiate and maintain sleep during the day, with the exception of a small window in the mid-afternoon, which is used by siesta cultures.
- Does sleep loss cause weight gain?
- Is sleep deprivation lethal for humans?
- Are polyphasic sleep schedules effective?
- How much sleep must you lose to negatively affect immune function?
- Could we one day develop technologies or drugs to supplant the need for sleep?
- Why do we sleep lying down?
- Does sleeping position affect bone growth?
- What determines when we change positions during the night?
- Why is insomnia so common these days?
- Transient insomnia is for a period of up to a week. This is experienced by virtually everyone at some point in life, due to stress, illness, etc.
- Acute insomnia is for up to a month.
- Chronic insomnia is for longer than a month.
- Shift-work. The timing of the human circadian clock is set by light. Those engaging in night shift-work are usually unable to fully adapt to the work schedule, due to strong effect of the natural light cycle, and the tendency to revert to more normal schedules on free days. The circadian clock is not able to very rapidly change its timing (this is why jet-lag occurs) and it strongly promotes sleep during what it considers to be the night. Shift-workers are therefore commonly trying to sleep at a time when the circadian clock is not promoting sleep.
- Use of artificial light and light-emitting devices. The human circadian clock is acutely sensitive to light during nighttime. Light before bed suppresses natural melatonin production and also delays the circadian clock, resulting in the body wanting to go to bed later on both that night and subsequent nights.
- Do biorhythms have any scientific basis?
- What is actually happening in the brain to make you sleepy the longer you are awake?
- Why must eyes be closed to sleep?
- What is the difference between sleeping for a certain period of time and lying in bed awake with your eyes closed?
- Is it possible to adapt to daytime sleeping?
- Do all animals sleep?
- Can falling asleep on my arm be dangerous?
- Why does inadequate sleep cause dark circles under the eyes?
- Decreased cognitive function. After 24 hours awake, your performance is comparable to a blood alcohol concentration of 0.10%. Cumulative sleep loss also adds up: Two weeks of 6 hours in bed per night results in performance levels similar to being awake for 24 hours. Two weeks of 4 hours in bed per night results in performance levels similar to being awake for 48 hours.
- Decreased immune function. People who sleep less than 7 hours per night are on average 3 times more likely to develop an infection after exposure to the common cold virus than those who sleep 8 hours or more.
- Increased risk of coronary heart disease and cardiovascular disease for those who sleep unusually short or long. The same is true for all cause mortality.
- Impaired ability to process glucose and release insulin. Sleep loss studies have shown that these aspects of metabolism are impaired. Restriction of sleep to 5 hours per night for 1 week can result in a prediabetic state in otherwise healthy young adults. This may also ultimately lead to an increased risk of developing type 2 diabetes and impaired glucose tolerance.
- Increased hunger and likelihood of obesity. Reduced sleep results in higher levels of the hormone ghrelin (which signals hunger) and lower levels of the hormone leptin (which signals satiety). Sleeping less leads to greater food intake, increased weight gain, and greater risk of obesity.
- Are we meant to sleep in 8 hour blocks?
- Light has a direct alerting effect that makes it difficult to go back to sleep;
- Light exposure near or after bedtime suppresses the secretion of melatonin, which has cancer-protective properties, and also helps you to sleep;
- Light at that time causes a phase delay shift of your circadian clock, effectively moving you to a later schedule and making your body want to wake up later and go to bed later the next day. Room light, or even screen light, is enough to cause all of these effects. If you really want to live on such a schedule, you need to accept candlelight or dimmer during the night between sleeps, which most people are not happy to do.
- What happens if I leave the light on at night?
- Do dreams occur in real-time?
- Is dream analysis valid?
- What determines our dream content?
- Is REM sleep the only stage that matters?
- How long does it take the brain to transition from sleep to wake?
- What is happening when I push through sleepiness?
- Why do fevers cause strange dreams?
- Do stressful dreams have the same effect on the body as stressful situations in real life?
- Does it matter which stage of sleep you wake from?
- Did people used to sleep earlier than they do today?
- Do some people just need less sleep?
- If you sleep without an alarm clock, do you sleep the exact amount of time you need?
- Is it better to get a tiny bit of sleep or to get no sleep at all?
- Why don’t we roll off our beds at night?
- Does lucid dreaming exist and is it different from regular REM sleep?
- Do babies dream?
- Very similar brain activation during sleep to humans when they are dreaming.
- REM sleep behavior disorder in humans is associated with failure to lose muscle tone during REM sleep, causing people to act out their dreams. Animals with lesions in the same part of their brain also appear to act out their dreams.
- What causes sleep talking?
- Could humans live on a planet or a schedule with a period different from 24 hours?
- Do other animals dream?
- They have REM sleep, like us, which is where we do most of our dreaming.
- They have apparent replay of memories.
- There is a sleep disorder in humans called REM sleep behavior disorder, which is essentially a failure to lose muscle tone during REM sleep. As a result, people physically act out some of their dreams. If the regions involved in generating muscle atonia are lesioned in other mammalian species, they too appear to act out their dreams.
- Why don’t bears lose muscle mass while hibernating?
- Why do you start to feel better in the morning after staying awake all night?
- Is sleep just a byproduct of the fact that Earth rotates?
- What is unihemispheric sleep?
- What is the difference between sleep and coma or unconsciousness or anesthesia?
- How can a sleep schedule be shifted earlier?
- Does taking melatonin actually work?
- Is jet lag largely unavoidable?
- Is it more useful to take a short nap, to help cope with a shift in sleeping pattern, or is it better to stay awake (or lie in bed, depending on what you're trying to do)?
- How does alcohol affect sleep?
- What is ‘sleep’ in the eyes?
- How long does sleep debt build up for?
- Do people ever sneeze while asleep?
- Why do we prefer a dark environment for sleeping?
- Why does sleep loss cause headaches?
- Does sleep deprivation affect neurotransmitter levels in the brain?
- Norepinephrine
- Serotonin
- Dopamine
- Histamine
- Orexin
- Increased serotonin turnover
- Increased extracellular serotonin
- Increased dopamine concentration in cats and rats
- Widespread changes in neurotransmitter receptor function and expression
- Increase in histamine concentrations during recovery but not during deprivation itself
- Increased activation of orexin neurons
 Yes, in fact there are many such studies.
Yes, in fact there are many such studies.
Epidemiological studies, including this meta-analysis have reported significant associations between sleep duration and weight.
Longitudinal studies have also found associations between short sleep and weight gain, although these two recent reviews suggest that the evidence is currently strongest for children.
As to why people gain weight as a result of insufficient sleep, we think that there are a few factors involved. Metabolism is actually lower by ~30% during sleep compared to lying still and awake, so you might hypothesize that sleep loss should result in weight loss, all else being equal.
However, it turns out that sleep deprivation reduces levels of leptin (a satiety hormone released by fat cells) and increases levels of ghrelin (a hunger hormone released by the stomach). This is true both in the general population, in those with chronic insomnia, and in healthy individuals who are experimentally sleep deprived.
Following sleep deprivation, people tend to over-compensate, eating more food than is needed to maintain energy balance. This is thought to be the reason for net weight gain. In addition, sleep deprivation impairs glucose metabolism and insulin sensitivity. Indeed, experimental studies in healthy young adults have shown that sleep deprivation and/or circadian misalignment can result in a pre-diabetic state.
Being overweight is also the primary risk factor for developing sleep apnea, which can lead to an unfortunate feedback loop in which poor sleep leads to weight gain and weight gain leads to poor sleep.
We don't know whether total sleep deprivation in humans leads to death. The longest any individual has undergone total sleep deprivation under controlled laboratory conditions is ~11 days. Under those conditions, cognitive function is greatly impaired along with other physiological functions, but there is no sign of any syndrome that may lead to sudden death.
Additionally, it's difficult to maintain total sleep deprivation over long periods of time. With increasing time awake, elements of sleep (including increased EEG theta power) or microsleeps begin to enter wake with increasing frequency.
Fatal familial insomnia (FFI) is an example of a disease in humans where individuals are unable to sleep and eventually die. However, it is not known whether death is due to sleep loss per ser, or to the prion disease.
The best known example of sleep deprivation leading to death is from studies in rats where the rats lived on a flat circular disk above a pool of shallow water. Rats were paired, with two on opposite sides of a disk, separated down the middle by a barrier. One of the rats was constantly monitored by EEG. If they fell asleep, the disk began slowly rotating, meaning both rats would need to wake up and begin walking so as not to fall off into the water. The other rat was therefore free to take naps whenever the monitored rat was awake. This method results in a loss of up to 90% of sleep for the monitored rat and about 30% for the other rat.
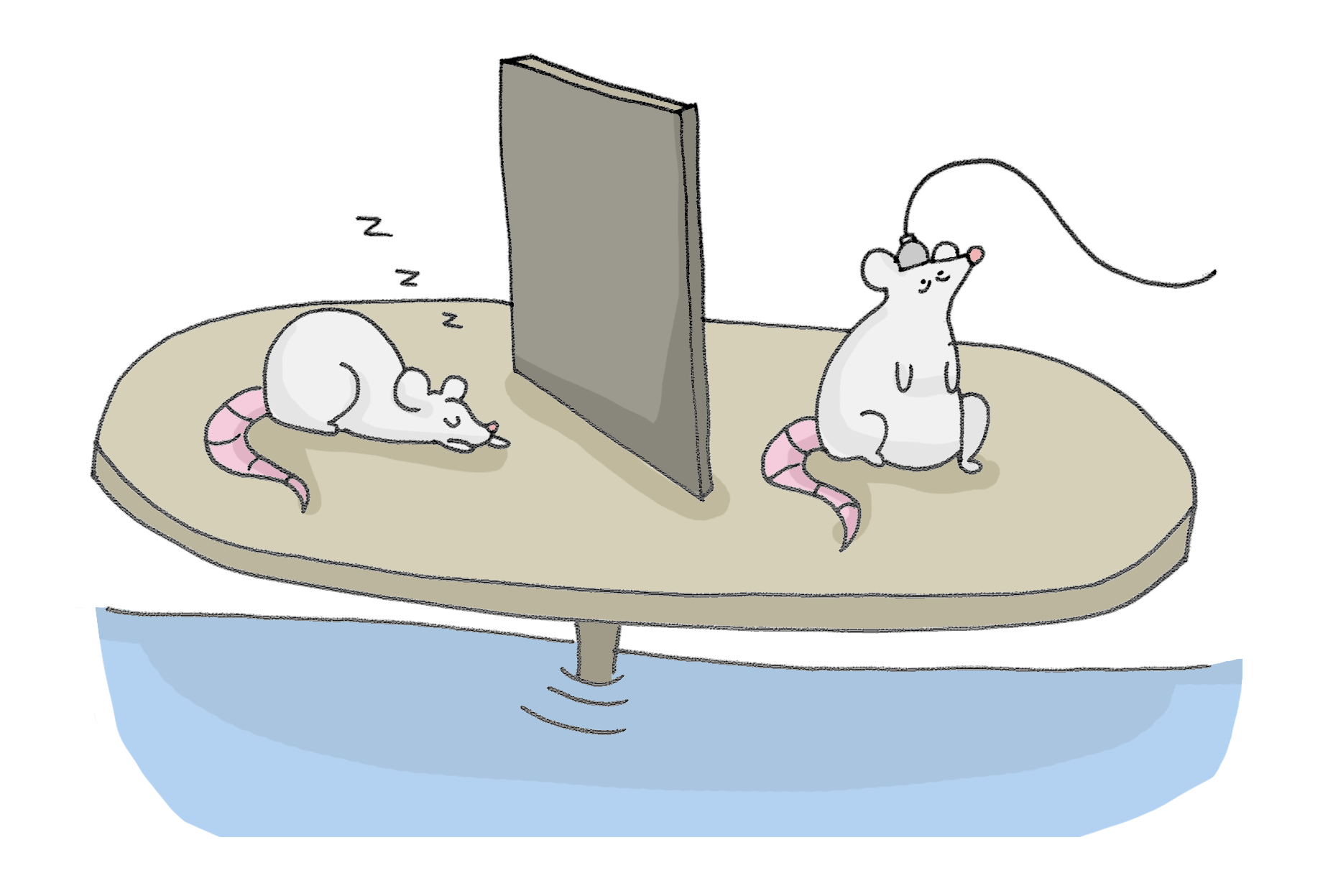 Both rats therefore undergo a similarly stressful procedure, but the monitored rat dies after a couple of weeks, whereas the other rat has no serious problems. The cause of death under these conditions is still unclear, but evidence points towards impaired immune function and negative energy balance, which may lead to systemic bacterial invasion.
Both rats therefore undergo a similarly stressful procedure, but the monitored rat dies after a couple of weeks, whereas the other rat has no serious problems. The cause of death under these conditions is still unclear, but evidence points towards impaired immune function and negative energy balance, which may lead to systemic bacterial invasion.
Some of these physiological responses -- including impaired immune response -- are a hallmark of sleep deprivation. However, death due to sleep deprivation has not been observed in other species, or even in rats sleep deprived in other ways. Quoting from a recent review:
Sleep deprivation in pigeons by the same technique used in rats is not lethal and produces none of the metabolic and thermoregulatory changes observed in rats [16]. Human sleep deprivation for as long as 11 days and chronic sleep restriction does not produce even the earliest signs of the autonomic changes seen in rats undergoing sleep deprivation by the ‘disk-over-water’ technique. Body temperature tends to fall in sleepy humans, rather than rising as it does in the initial stages of sleep deprivation in rats [17,18]. Humans whose sleep is reduced for long time periods tend to gain weight, rather than lose weight as rats do under 70%–90% sleep deprivation conditions [19]. Fatal familial insomnia, a rare genetic condition reported in humans, is not analogous to the disk-over-water method of sleep deprivation [13] because it is characterized by massive brain degeneration and autonomic dysregulation [20].But if we're talking about sleep deprivation and death, we should be sure to touch on selective brain lesions. The brainstem and hypothalamus contain many neurons involved in the regulation of wake and sleep. From 1915-1924, there was an epidemic of encephalitis that caused damage to many brain regions, including these sleep and wake regulatory neurons. This was studied by von Economo, who found that depending on the area of damage, the encephalitis caused different types of sleep disorders, including profound lethargy, profound insomnia, and inversion of sleep/wake cycles.
Later experiments were able to localize these neurons and identify their specific functions and circuitry. In 1946, Nauta et al. lesioned some of these brain regions, resulting in either constant sleep or constant wakefulness. Here is what they report:
The normal difference in activity between day and night -- established by Szymanski who in a space of 24 hours registered an average of 14 hours of sleep distributed over 10 period, which were longer and more frequent during the day than during the night -- was in this way found to have disappeared completely, the rats being awake whenever they were observed. The animals showed a normal interest in their environment. Their general condition was excellent at first and they spontaneously took food and drink. Soon, however, their state deteriorated, which is not surprising considering the large amount of sleep to which the rat is accustomed. After a period of 24 hours the sleepless rats usually began to show symptoms of fatigue. They did not eat or drink of their own accord and their interest in the surroundings decreased. Symptoms of sham rage, if present, persisted. In spite of the fatigue and even of the succeeding exhaustion during which the gait became unsteady, sleep was not forthcoming, the opened eyes and the spontaneous activity proving that the animals were awake. After a period averaging three days the exhausted animals fell into a state of coma which soon ended in death. A return of the sleeping capacity was never observed in any of the animals.So it's not known what the cause of death was, but it is an interesting experiment. It's also worth noting that a more recent experiment involving lesions of this brain region and EEG recordings found only a 60% decrease in NREM sleep that persisted for at least three weeks without death, although the lesioning method was different.
We did not observe hypothermia in sleepless rats, nor did these animals develop purulent infections of mucous membranes.
TL;DR: We don't know if sleep deprivation is lethal for humans or other species. In some cases (disk-over-water or brain lesion), it seems to be lethal in rats. That may be due to impaired immune function, but we don't know for sure.
No, not at all.
Adopting a "polyphasic" schedule (where polyphasic is here taken to mean naps evenly distributed across the day) is in essence doing battle with your own biological drives. You must attempt to sleep during the day, when the body is strongly promoting wakefulness, and attempt to stay awake during the night, when the body is strongly promoting sleep. The net result of such a schedule is chronic sleep restriction.
 Or, in more detail: Seven reasons why attempting polyphasic sleep is a bad idea (for humans).
Or, in more detail: Seven reasons why attempting polyphasic sleep is a bad idea (for humans).
1. NREM/REM cycles
Sleep in adult humans is characterized by an approximately 90 min oscillation between rapid eye movement (REM) and non-REM (NREM) sleep stages. Unless you are REM sleep deprived, you will almost always enter NREM sleep first during a nap, reaching REM sleep later. While we don't yet know the precise function of the NREM/REM sleep cycle, we do know that fragmenting sleep and/or decreasing REM sleep results in less restful sleep and more waking impairments in neurobehavioral function.
2. Circadian rhythms
With the exception of a small window in the mid-afternoon (used by siesta cultures), it is extremely difficult to rapidly fall asleep when trying to nap during the day, without a background of severe sleep deprivation. For this reason, people who try to distribute their sleep in naps across the day have great difficulties achieving a good total amount of sleep. This is the same reason shift-workers experience enormous difficulties getting sufficient sleep -- they are typically trying to sleep at the 'wrong' circadian phase, and often in the presence of light (which promotes wakefulness).
3. Sleep inertia
When you first wake up, you tend to experience a groggy feeling for up to an hour or two, called 'sleep inertia'. Sleep inertia occurs following any naps longer than about 20 min. Ordinarily, you only have to deal with sleep inertia once per day -- in the morning. Distributing sleep into multiple long naps would mean that you spend much of your day impaired by sleep inertia.
4. Light
The circadian system has evolved to expect light during the day and darkness during the night. Your circadian clock is therefore exquisitely sensitive to light exposure during the night. People who have periods of wakefulness during the night typically use artificial light, which completely suppresses the normal nighttime release of the hormone melatonin. Melatonin not only helps you to get to sleep, it also has many other important roles, including as an anti-oxidant. Night-shift work has been named by the WHO as a probable carcinogen, and light-induced suppression of melatonin is currently considered one of the most plausible mechanisms underlying this.
5. Insufficient sleep
Because of the circadian drive and other confounding factors, it’s harder to fall asleep on a polyphasic schedule. The result is insufficient total sleep time across 24 h, unless one allows 12+ h of time in bed per day, which completely defeats the purpose of such schedules. It’s important to note that 6.5-7.5 h sleep is definitely insufficient in terms of optimal cognitive performance, at least for the average population.
6. Misery
Participants in polyphasic sleep studies really don't like being forced to live on these schedules, because they are made to fight against their own biological urge to sleep during the night. Interestingly, if you read the blogs of people who actually try to make these schedules work, they usually have to come up with activities to help them stay awake during the time of highest biological sleep drive (around 5am).
7. Health concerns
In general, any schedule which desynchronizes sleep from underlying circadian rhythms is suspected to be bad for your health. Most of this has come from work looking at shift work, where multiple poor health outcomes have been studied. The most common outcome under investigation right now tends to be various cancers (examples here and here), though cardiovascular and metabolic outcomes have seen some associations as well. Some of this has been substantiated through animal models of shift work, in addition to "jet lag" models (such as here) and by ablation of the SCN (the suprachaismatic nucleus - the central pacemaker for mammals).
This is the biggest flaw with many of the 'evenly divided' polyphasic sleep schedules - they ignore the fact that sleep is closely connected with underlying circadian processes, and tends to be a well-regulated process. The two process model is still one of the most commonly considered overall models for sleep and its connection to the circadian system. Attempting to decouple sleep and circadian processes tends to result in poor health (the prior paragraph). In fact, most people we do see these sleep patterns in most often are those with attenuated rhythms and otherwise poor health (as is often the case in various dementias).
Many proponents of these polyphasic styles of sleep forget what the original purpose of these alternative schedules is. The point, at least when they were developed, was as an alternative for persons that required constant vigilance (such as solo sailors) and could not get more than 30-60 minutes of rest at a time. The idea is to ameliorate some of the more severe cognitive deficits to sleep deprivation. They were almost never meant as a substitute for a more natural, free-running sleep schedule.
Pretty much right away (after 1 night of sleep deprivation); see here and here.
 Sleep has been shown to improve functioning of the immune system, and inadequate sleep results in greatly impaired immune function. To give one interesting example, in a study a few years ago, a bunch of healthy participants were exposed to the common cold virus using a nasal spray. They were then observed to determine how many developed an infection.
Sleep has been shown to improve functioning of the immune system, and inadequate sleep results in greatly impaired immune function. To give one interesting example, in a study a few years ago, a bunch of healthy participants were exposed to the common cold virus using a nasal spray. They were then observed to determine how many developed an infection.
Interestingly, those who slept an average of less than 7 hours per night in the two weeks preceding the exposure were approximately 3 times more likely to develop an infection than those sleeping an average of more than 8 hours per night.
There are now many other studies linking sleep to the immune system; see, for example these two.
Could we block the urge to sleep with pharmaceuticals? Quite possibly, yes. We have a reasonably good understanding of the neurotransmitters that promote different states of arousal. These can be manipulated (e.g., using modafinil or amphetamines), although with serious side-effects. We are also developing an understanding of the substances that accumulate in the brain that drive sleep, e.g., adenosine, IL1, prostaglandin D2, and NO.
Caffeine works by temporarily reducing the effects of adenosine by acting as a competitive antagonist. We also understand the basis for the circadian clock, which promotes sleep at night and wake during the day, and in the future it could potentially be manipulated. But could we somehow substitute for the function of sleep with pharmaceuticals while maintaining normal wakefulness? It seems unlikely at the moment.
Don't forget that sleep serves fundamental functions for all the other systems of the body. Even supposing we could keep the brain in a perpetual state of wakefulness, we would not be addressing the roles of sleep/wake cycles in normal immune function, metabolic function, cardiovascular function, growth, protein synthesis, etc.
If it were possible to maintain consciousness while performing all the functions of sleep, there would be little reason not to evolve that ability. The only plausible reason would be to keep you out of trouble by forcing you to lie unconscious rather than interacting with your environment. The argument being that it's safer and/or more efficient to behave this way. However, many species sleep in the open and are more vulnerable by virtue of being unconscious.
 We therefore think that the processes that occur during wake and sleep are fundamentally incompatible on some level. Brain activity is certainly very different between these states. The argument then is that it is necessary to take the network 'off-line' to perform certain types of maintenance.
We therefore think that the processes that occur during wake and sleep are fundamentally incompatible on some level. Brain activity is certainly very different between these states. The argument then is that it is necessary to take the network 'off-line' to perform certain types of maintenance.
Cetaceans (e.g., dolphins) provide compelling evidence for this, and show an alternative strategy. They cannot afford to fall asleep completely, else they could drown or be predated. They get around this by sleeping unihemispherically -- switching one half of their brain off at a time.
Perhaps we can develop a similar strategy to decouple the sleep/wake patterns of different brain regions, although who can say what type of conscious experience would ensue, or whether it would be in any way preferable to how we naturally sleep. Alternatively, there may turn out to be ways to make the processes that occur during sleep more 'efficient'. In any case, we are some way from achieving anything remotely like this, so it's all just speculation at this stage.
There is a GABA-based motor suppression circuit in our brains that relaxes most of our skeletal muscles (atonia) during sleep. This is thought to serve a few purposes, one of which is to keep us from acting out our dreams and walking over a cliff, falling out of our tree, etc. This means that we cannot fully sleep while standing up- it's also why people get "the nods" when they are fighting sleep deprivation. The atonia in the neck and back muscles cause the head to fall under gravity, inducing a panic response from the vestibular system in the ear and waking the person back up.
It's also much easier for the body to sleep while relaxed and horizontal. The metabolic load is lower, the water column of the blood vessels isn't as pressurized, and the motor neurons controlling posture don't have to work.

Animals that do sleep vertically either have ways to minimize energy use (bats, for instance, don't need strong muscles to hang from their feet because their legs are built with lever systems to lock their toes when under load) or trade the energy spent on sleeping standing up for better predator evasion (i.e., it's easier to run when you hear a predator if your muscles aren't atonic and poorly perfused).
The horizontal position represents the lowest energy state your body could be in. First, in this position your heart will work less to circulate blood, as it will not be working against gravity to any large extent. Also, it is the safest, since your center of mass is lowest in this configuration.
One thing which would problematic about vertical sleeping for humans would be the stress which would be put on the one-way valves in the veins in your legs, which allow blood to pump against gravity. When they become incapacitated it causes swelling, varicose veins, etc. People who spend long periods of time sitting or standing tend to have more problems of those types, so regularly sleeping upright would probably be particularly damaging.
Yes, actually.
There is a cultural practice in Asia that favours supine-sleeping (versus prone-sleeping in North America) with measurable differences. Something called the Cranial Index (basically how wide your head is) is used to track infant cranial measurements and Asian children that sleep supine generally have "wider" heads than their American counterparts, which is termed "brachycephaly" ("short head") when their CI is greater than 0.81. Contact area with the bed seems to be the cause of this (back of head for supine sleepers vs. side of the head for prone sleepers).
The body has a number of bony prominences, which are areas where bone comes up close to skin level, such as the heels, the sacrum/coccyx, and the shoulder blades. As you sleep immobile, pressure builds on the skin beneath these bones and will eventually cause pain, numbness and then skin tissue damage/death if the pressure isn't removed.
Changing position shifts body weight off some prominences and onto others. Your brain decides when to move based off cues from the nerves in the skin under pressure.
In immobile people in hospitals there is a very high risk of developing pressure or decubitus ulcers for this reason - they can get horrible fast and every measure is taken to prevent them. Google that if your stomach is strong.
Also, sleep cycles play an important role: The muscles of the body are only paralyzed during rapid eye movement (REM) sleep. Muscle activation, including rolling over, as well as parasomnias such as sleep talking and sleep walking, can occur while people are in non-REM sleep.
 Across a night, it's very common for people with perfectly normal sleep to have 20+ brief arousals and to have a major change of body posture 10+ times in a night. This study reports an average of 20.1 awakenings per night in healthy young adults, 22.9 in middle-aged, and 27.9 in older adults. You often don't remember these; partly because short-term memory is poor just after awakening, and partly because many of these movements happen without awakening at all.
Across a night, it's very common for people with perfectly normal sleep to have 20+ brief arousals and to have a major change of body posture 10+ times in a night. This study reports an average of 20.1 awakenings per night in healthy young adults, 22.9 in middle-aged, and 27.9 in older adults. You often don't remember these; partly because short-term memory is poor just after awakening, and partly because many of these movements happen without awakening at all.
As to why we switch sides, there is no definitive answer to that. Plausible hypotheses would include comfort (it can be painful to lie on the same arm all night) and ease of breathing (it is harder to breath while lying on the back, because the airway loses some muscle tone during the night).
Insomnia is extremely common today, and, yes, it is common worldwide. When talking about this, it is important to draw the distinction between the different types of insomnia.
 Insomnia is medically diagnosed based on the inability to fall asleep, maintain sleep, or feel rested by sleep. This should be the case despite adequate opportunity to sleep, and should manifest with daytime impairments. Using that strict definition, there is thought to be a prevalence of about 5-10% for chronic insomnia.
Insomnia is medically diagnosed based on the inability to fall asleep, maintain sleep, or feel rested by sleep. This should be the case despite adequate opportunity to sleep, and should manifest with daytime impairments. Using that strict definition, there is thought to be a prevalence of about 5-10% for chronic insomnia.
Insomnia can have many causes. Often people use primary insomnia to mean insomnia that has no known underlying cause, and secondary insomnia to mean insomnia that stems from some other medical problem, e.g., pain.
Others suffer from sleep state misperception, otherwise known as subjective insomnia, where they objectively appear to sleep based on polysomnography but do not feel feel that they are sleeping.
In general, insomnia is more prevalent in women than in men and more prevalent in old age. There are theories as to why these things are the case, including sex differences in the intrinsic properties of the circadian clock and age differences in the ability to maintain consolidated NREM sleep, possibly due to loss of sleep-regulatory neurons and changes in circadian regulation of sleep with age.
It is difficult to know whether rates of insomnia are on the rise, since there have not been stable diagnostic criteria used consistently over a long period of time. Nevertheless, we do know that many behaviors in modern society negatively affect sleep hygiene, leading to more difficulty falling asleep and maintaining sleep. These problems stem mostly from two causes:
Biorhythms have no scientific support whatsoever. For those unfamiliar with the idea, it was a pseudoscientific fad that claimed to predict your "physical", "emotional", and "intellectual" state, assuming that the three factors oscillated with 23, 28, and 33 day periods, respectively, beginning at your birth. This can be put in the same basket as astrology. There is absolutely no basis for those oscillatory periods or even for there to be simple rhythms in those factors (which are ill-defined to begin with).
However, there are many biological rhythms that definitely do exist in humans and other organisms. The ones you may be most familiar with are the circadian (~24-h) rhythm and the menstrual (~29-d in humans) cycle. Both of these are endogenously generated, meaning they will persist even in an environment free of any time cues.
There are two factors that primarily regulate how tired or sleepy you are across the day.
The first is your circadian rhythm, which for a diurnal (day-active) organism promotes alertness during the day and sleepiness at night.
The second is the accumulation of sleep regulatory substances in the brain with time awake. These include adenosine, cytokines, prostaglandin D2 and some other molecular factors. The longer you are awake, the more these accumulate. This is usually called the "sleep homeostatic drive".
Smaller mammals do tend to cycle more quickly between wake and sleep across the day than larger mammals. The reason for that is not entirely clear, but it is possibly linked to metabolism via the sleep homeostatic drive, i.e., those sleep regulatory substances may accumulate and clear more quickly in smaller mammals. That's just a hypothesis at this stage though.
There is, however, some evidence to link sleep to maintaining ATP levels in the brain. Other lifestyle and environmental factors can also influence levels of alertness, e.g., light exposure, diet, and exercise.
The visual input to the brain is one of the strongest drivers of the reticular activating system. This system includes the pedunculopontine nucleus as well as the Nucleus Basalis of Meynert, and is responsible for the bulk of the arousal effects in the brain. Short answer - if you have visual input, you have strong input to the brain's arousal centers, and that of course biases your brain to keep you awake.

The other senses have inputs too, just not as strong, and they also have documented strong attentional influences on primary sensory cortex that appear to be lacking in vision. Short answer - it appears right now that you can gate touch and hearing to much lower levels than you can vision (why is an interesting question but I could only speculate), so they may impact the reticular activating system as strongly when you are drowsy.
Some people do sleep with eyes open, but their sleep is more fragmented and they often suffer from light sensitivity and dry eyes.
We think there are a few reasons for this. First, reducing environmental stimuli helps the brain to enter and maintain sleep. This is for the same reason that it is easier to fall asleep in a quiet dark environment than a noisy bright environment. Closing the eyes helps to reduce incoming environmental stimuli, which changes brain activity (increases alpha power) and makes it easier to fall asleep. Additionally, having the eyes closed during sleep stops them becoming dry.
The fact that it is possible to sleep with eyes open is probably largely down to modulation of incoming stimuli by the thalamus. The thalamus is a region of the brain involved in relaying environmental stimuli to the cortex. The thalamus enters a different mode of activity during sleep, which is partly why the brain is less responsive to environmental stimuli and why it is even possible to fall asleep with eyes open.
The answer was found very recently by neuroscientists. You see, neurons in the brain use a lot of energy, and they don't have enough space to store excess chemical energy (in the form of glucose or lactate). So neurons get excess energy from astrocytes. Astrocytes store chemical energy, and during the day, when our neurons are energy-starved, molecules of lactate will transfer to the neurons, providing them metabolic energy. The energy reserves of the astrocytes become depleted during a day's mental activity.
When we sleep, the chemical energy reserves of astrocytes are replenished. This has been hinted at by experiment. Example: two groups (plus control groups) undergo intense physical exercise and intense mental exercise, respectively. Then they sleep. The group who exercised physically subsequently needs a normal amount of sleep (equivalent to the control group), while the group who underwent mental exercise needed more sleep. Thus we can conclude that neural activity (specifically heightened metabolic activity) is related to sleep.
How does this happen? When astrocytes run low on energy, they release adenosine, a neuromodulator. Adenosine is an inhibitory neuromodulator. It stops neurons from firing, presumably stopping them from using more energy than is available. As the day wears on, adenosine levels rise in the brain. After sleep, adenosine levels return back to where they were. It is hypothesized that adenosine causes most of the physical effects we collectively call "sleepiness": difficulty moving, clouded thoughts, laziness, etc.
Keep in mind that the above is just a physical explanation and somewhat speculative. It's from the textbook Physiology of Behavior by Carlson. Highly recommended.
If you are tired because you just worked out, then sitting down to rest will help you feel better (we do it all the time). Sitting down or laying down, though, will not affect sleepiness.
 Exercise does affect sleep (after exercise, you tend to have more slow wave sleep), however, this is related to the rise in temperature during exercise, not the physical exhaustion of the exercise. If you were to blow a misting fan on a person running on a treadmill so that their body temperature does not rise, you will not see a change in sleep.
Exercise does affect sleep (after exercise, you tend to have more slow wave sleep), however, this is related to the rise in temperature during exercise, not the physical exhaustion of the exercise. If you were to blow a misting fan on a person running on a treadmill so that their body temperature does not rise, you will not see a change in sleep.
Researchers have done long term bed rest studies (weeks at a time not getting out of bed for anything) and have found that sleep does not change. The sleep of people with quadriplegia (and therefore do not have much physical movement) is also not substantially different from a person that is not injured. Therefore, sleep does not seem to be for physical recovery.
On the other hand, if a person has a very mentally stimulating day, you will likely see an increase in slow wave sleep at night. Even if you place a person's hand on a vibrating platform so that is activates their somatosensory cortex, you will see a local increase in slow wave activity in the somatosensory cortex. So it seems likely that sleep is for brain recovery.
Would laying on the bed without sleep do anything? Yes, if your legs were tired, much like sitting down, they would probably be refreshed (though likely quite stiff if you were still the whole time). But you would be sleepy, just the same as if you stayed up all night reading a book. The one difference between being in bed with your eyes closed and reading is book is that you most likely cannot lay in bed for 8 hours with your eyes closed and fail to fall asleep. In the Maintenance of Wakefulness Test, where you are asked to stay awake for 40 minutes in a bed in a dark/quite room, 40 to 60% of people without sleep disorders will still fall asleep. People, especially those with insomnia, greatly under report the total amount of sleep they receive each night because they do not perceive short sleep periods. You would have to be unusually well rested to make it 8 hours with your eyes closed without falling asleep.
Different species have evolved to be active during different parts of the day/night cycle -- this is called the animal's temporal niche. Nocturnal (night-active) and diurnal (day-active) species have evolved different traits to improve their functioning during the day or the night. For example, highly nocturnal species typically have higher rod:cone ratios and larger pupils to capture more light.
Humans have evolved to be diurnal, getting most of our sleep at night. There are some inter-individual differences in the properties of the circadian clock and other aspects of sleep regulation that result in individuals naturally going to bed and waking up at different times, but not to the extent where anybody could be considered nocturnal. Some people choose to adopt a nocturnal schedule (e.g., night-shift workers), but this is in conflict with our physiology, making it very difficult to fully adapt.
Blackout curtains, eye masks and earplugs can whelp. Make sure to put your phone on silent and make rules with your family/friends that no one bothers you during your sleep time. You also want to follow good sleep hygiene and avoid downing a bunch of coffee toward the end of your shift (though this may be problematic if you have to drive home after).
The family and friends part is very important. They have to realize you are unavailable during that time of the day. They cannot ask you to help them take the car to the shop because you are home, just like they would not ask someone else to do it at 3am. Most of the research will say people cannot effectively always work the night shift. But if you look at, for example, people that work on an oil rig, they can work 7-14 night shift in a row without too much problems. The difference is that once they are done, they can go to sleep. No kids to see off in the morning, no friends calling at 10am, etc. Their big problems come when they go back home and try to readjust to their family's schedule.
If you are going back and forth between day and night shift, there are a whole host of different problems. You really want to have at least 2 days off after a night shift to get back into a normal rhythm. You also do not want to do night shift, day off, night shift because you will probably want to interact with the outside world on that day off and that will screw you up as well.
Also, if possible, get home before the sun rises. The sun is your body's cue to wake up, so driving home in the morning sun will make it harder for you to go to sleep. If that cannot be avoided, make sure to wear dark sun glasses to minimize sun exposure. Melatonin supplements can also help.
This all depends on your definition of "asleep." But that would be a disappointing and stupid answer, so I'm gonna develop it by examining possible definitions of "sleep" and what would fall under each.
It seems improper to call it "sleep" just because they have cycles of activity/inactivity - that's just a diurnal rhythm. If we define "sleep" as "having a diurnal rhythm with an inactive phase," the answer is very broad. Jellyfish/cnidarians and flatworms/platyhelminthes have cycles of activity/inactivity, and in fact so do many species of bacteria. So that would pitch our "most recent common ancestor" back to the divergence of eukaryotes from prokaryotes.
Another question is: "what is the most recent common ancestor of all organisms that can be awake?" So here we need to define "awake," and I've done so provisionally as "active, variable thinking".
Specifically, this means that it's not "thinking" if an animal is following reflexes and pre-determined behavior modes. This is convenient, because it means we can define insects as "not awake," and if we couldn't we'd have to say that "the most recent common ancestor of all organisms that require sleep" is the most recent common ancestor of vertebrates and invertebrates. That's enteropneusta, 540 million years ago, and that's not very informative.
So we should define sleep more complexly, and here's my proposal. An animal needs to be multicellular (sponge), have neurons (jellyfish/cnidarians), have a central nervous system which processes complex behavior patterns, and swap between modes of active, variable "thinking" (awake), and passive neural maintenance (sleep).
So if we go down the vertebrate path, we get phylum Chordata, including sea squirts/tunicates, lancelets/amphioxus, jawless fish/agnatha, sharks and rays/chondrichthyes, bony fish/osteicthyes, and then the tetrapods, reptiles, birds, and mammals. Fish don't have REM sleep (dreaming), nor do they show novel learning, so I would put them in the "don't sleep" category (this is another point where it'd be perfectly understandable to start disagreeing with me), but they do have cycles of behavioral activity/inactivity. If you want to define "sleep" as "having a time when it's hunting and a time when it's not," fish fall under this category, but then again, so do insects, so we have to go all the way back there.
If we want to define "sleep" as "having a circadian rhythm which includes a period of passive neural maintenance for learning, and associated paralysis," we have our terrestrial tetrapods (for whom sleep is easiest anyway - they can lay down). Here we could get into a disagreement over whether lizards/snakes/turtles/alligators/reptiles do not seem to demonstrate novel learning, but birds and mammals definitely do. But lizards are more closely related to birds than mammals are, so that saves us the trouble, and we get our answer.
The most recent common ancestor of all organisms that require sleep, is the most recent common ancestor of mammals, and birds. That'd be the proto-tetrapod, and last I heard that was considered to be acanthostega.
This phenomenon is caused by the pinching of a nerve, typically by pressing it up against a bone or other hard object in the body. Pinching a nerve disrupts a small area of nerve conduction where the pinch took place (think kinking a water hose). It takes a while for this area to properly set up its electrochemical gradient again, hence the delay in regaining the nerve's abilities.
 Damage (e.g. cell death of muscles or nerve) could only occur if blood flow were to be cut off from an area for an extended period of time, which is a trickier thing to do (think tightly wrapping a rubber band around the end of your finger). The human vasculature is very good at finding detours in the body (called anastomoses) to make sure all areas get equally perfused. Awkwardly sleeping certainly isn't good in the long run, but unless you accidentally a tourniquet on your arm, you should be fine.
Damage (e.g. cell death of muscles or nerve) could only occur if blood flow were to be cut off from an area for an extended period of time, which is a trickier thing to do (think tightly wrapping a rubber band around the end of your finger). The human vasculature is very good at finding detours in the body (called anastomoses) to make sure all areas get equally perfused. Awkwardly sleeping certainly isn't good in the long run, but unless you accidentally a tourniquet on your arm, you should be fine.
It actually has a name: Saturday night palsy or honeymoon palsy. The name coming from either passing out on your arm or having someone sleep on your arm. The nerve is affected by direct compression, which usually only results in the arm being asleep for a while. However, if the compression is sustained for a longer period (which usually only is the case if you're passed out due to alcohol or drugs) the same direct compression of the nerve will lead to cell death in the part that is distal to the compression, i.e. not related to blood flow in the extremity. To explain it simply, nerves that don't get continuous signals from the spinal cord will die. The nerve sheath is intact though, and the nerve will regenerate, something like a couple of mm per day, so it takes a while before you have control over your arm again. You can learn more here.
The answers here are all speculative, and that's because nobody actually knows. If you do some google searches, you will find a lot of plausible but unsupported arguments for sleep deprivation causing vasodilation.
There's a recent review that mentions several physiological causes of dark circles under the eyes:
Histological characteristics of infraorbital darkening suggest that they are caused by multiple etiologic factors that include dermal melanin deposition, postinflammatory hyperpigmentation secondary to atopic or allergic contact dermatitis, periorbital edema, superficial location of vasculature, and shadowing due to skin laxity
It also mentions that sleep deprivation can contribute to this darkening, but it does not attempt to explain why that happens. There is certainly evidence to show that sleep deprivation causes changes in vascular function.
However, the exact mechanism underlying the dark circles under the eyes does not seem to be known. In short, they found that sleep deprivation alters a whole bunch of measures of vascular function, including heart rate variability, blood pressure, as well as of inflammation. This is in line with numerous other studies that have shown detrimental health effects of sleep loss.
Specifically,
The answer is: We're not entirely sure!
To start with, almost all mammals sleep polyphasically (i.e., multiple blocks of sleep per day). Monophasic sleep (i.e., one block of sleep per day) is unusual, but humans are not the only species that do it. So far as we know, the behavior is restricted to primates, though -- and not all primates sleep that way. Some also sleep biphasically (i.e., they have a main sleep block at night, and a shorter nap during the day, a la siesta cultures).
In modern human society, adult humans sleep almost exclusively monophasically. But it could be argued that this is due to electric lighting and standardized work hours. There is certainly a tendency towards increased sleepiness in the afternoon, which allows afternoon napping in some people. Many children nap, of course, but they tend to nap less as they move into adolescence and then into adulthood, as our ability to maintain extended wakefulness improves.
There was a book recently that gained a lot of attention called At Day's Close that argued that people in medieval times slept in two discrete chunks at night, i.e., split sleep. They would have a first sleep around sunset, then wake for a few hours, and then have a longer second sleep to dawn. This brought the idea of a split sleep pattern back into vogue.
It's still unclear whether this is our 'natural' sleep pattern, even if one can agree on a use for the word natural. The only real recent evidence to corroborate split sleep is a study in which people were put on schedules where they were in a lit environment for 10 hours per day, and put into bed in a completely dark room for 14 hours per day. Under these conditions, some of the subjects started to split their sleep into two chunks on many nights. Whether this is in any way related to what we should naturally do is questionable; it is perhaps a simulation of winter nights before the advent of electricity.
Other studies have observed villages where they do not have electricity yet, and found people sleeping into a single consolidated nightly block.
The problem with the split sleep schedule in the modern age is that you are likely to get artificial light exposure during the time that you are awake in the middle of the night. This is really terrible for several reasons:
There's certainly no existing evidence to suggest that split sleep is better than consolidated sleep, be that in terms of health or cognitive function. I should also note that there is definitely no evidence to support sleeping regimes that distribute sleep evenly across the day in naps (Da Vinci, Uberman, etc.). In fact, there is a wealth of knowledge to show that they are terrible.
Our bodies contain circadian clocks that strongly promote wakefulness during the day and sleep during the night. This makes it difficult to initiate sleep during the day, except for during a small window in the mid-afternoon (where people traditionally nap).
Polyphasic sleep regimes effectively put people on an ultradian sleep/wake cycle, i.e., shorter than 24 h. Under those conditions, there are times during the day when it is nearly impossible to fall asleep.
The result is insufficient total sleep time across 24 h, unless one allows 12+ h of time in bed per day, which completely defeats the purpose of such schedules. It is also interesting to note that such schedules disrupt the usual architecture of REM/NREM sleep cycling; whether that has a negative effect on performance, we don't yet know.
Also, participants really don't like being forced to live on these schedules, because they are made to fight against their own biological urge to sleep during the night. Interestingly, if you read the blogs of people who actually try to make these schedules work, they usually have to come up with activities to help them stay awake during the time of highest biological sleep drive (around 5am).
Again: 6.5-7.5 h sleep is definitely insufficient in terms of optimal cognitive performance, at least for the average population.

Your circadian clock will be affected! By how much depends on how much light you get.
Candlelight is ~1-10 lux
Room light is ~100-300 lux
Sunlight is ~1,000-100,000 lux
It seems like room light should be insignificant looking at that scale. But the response is nonlinear over the physiological range, such that 100 lux gives about 50% of the response that 100,000 lux would.
Now, the only light that matters is light that actually reaches the retina, since that's the only way for light to affect the mammalian circadian clock. The eyelids filter out over 95% of the light that matters, so a relatively dim light on during the night is unlikely to have much of an effect on either melatonin release or circadian phase.
But some people find light at night disturbing, and then they are not able to sleep as soundly. It is worth noting that the circadian system is particularly sensitive to light at the bluer end of the spectrum. Redder lights therefore have less effect.
Right now we don’t know for sure.
The problem is that we don’t have a good methodology for measuring the progression of dreams while people are asleep. Waking someone up to ask how long they have been dreaming is unreliable, since dreams often take peculiar non-linear leaps of time, and new memory formation is impaired while asleep (which is why people don’t remember most dreams). There’s also no way of telling exactly when the dream began. The entire narrative structure of dreams can be very disjointed and is very different from wake. The very question ‘What time-span did a dream cover?’ may not be a sensible one to ask.
One study woke people after they had been in REM sleep for 5 or 15 minutes and made them guess how long it had been, on the premise that dreams may have started when the REM sleep episode began. With very high accuracy, the subjects correctly guessed whether it had been 5 or 15 minutes. Unfortunately, dreams can also occur in NREM sleep, and we don’t know whether dreams persist across a transition between NREM and REM sleep. Also, that experiment did not allow participants to freely guess, they just had to go with the short (5 minutes) or long (15 minutes) category. Nevertheless, if the entire metric of time were altered in REM sleep relative to wake, you might expect some systematic error.
To truly answer the question, we would therefore need to use monitoring or imaging technologies that can somehow translate the brain’s activity into the actual mentations. On the large scale (using EEG), brain activity in REM sleep actually looks quite similar to brain activity in wake. It's certainly possible that the rate of mentation is very different in REM sleep, but the null hypothesis of no difference is sensible and it would take strong evidence to the contrary to prove that dreams are not perceived in real time.
 One piece of evidence that possibly supports dreams not being in real time (and which I suspect most of these ideas, like Inception come from) is from studies of place cells during wake and sleep. Place cells, as their name suggests, fire when you are in a particular place or thinking of that place. They are essentially your personal map of the world. When rats are learning to solve a maze, you can put electrodes into the hippocampus to measure when place cells are firing, and see them making new associations between parts of the maze and individual place cells.
One piece of evidence that possibly supports dreams not being in real time (and which I suspect most of these ideas, like Inception come from) is from studies of place cells during wake and sleep. Place cells, as their name suggests, fire when you are in a particular place or thinking of that place. They are essentially your personal map of the world. When rats are learning to solve a maze, you can put electrodes into the hippocampus to measure when place cells are firing, and see them making new associations between parts of the maze and individual place cells.
If you watch what those neurons do during subsequent sleep, they sometimes appear to fire in the sequence corresponding to moving through the maze, but they do so faster than the rat would move through the maze during wake. This could be interpreted as the rat dreaming about walking through the maze and dreaming in faster than real time. However, note that this is occurring during slow-wave (NREM) sleep, whereas most vivid dreams occurs during REM sleep. There have also been recent studies linking the order of firing of place cells to theta waves during REM sleep.
It's tempting but premature to make the leap from saying those cells are firing to saying that the rats are actually consciously perceiving those memories. We may instead be seeing offline testing/consolidation of memories, since we know sleep is involved in those processes.
Short Answer: No-- dreams probably have no valid analysis.
Long Answer: Dreams you remember and care about enough to discuss with a talk therapist probably do have meaning, but it's intensely personal and has far more to do with the fact you're having intense dreams and the "meaning" you ascribe to them while awake, not some meaning ascribed by a third party.
So, best example I can think of-- PTSD sufferers report unpleasant, recurrent nightmares. If you go back to your old war zone every single night and seek out a psychiatrist because of it, you might have PTSD.
I can't speak for psychologists, but for those in sleep research, Freudian dream analysis is today held in very low regard. From a physiological perspective, we have some understanding of the processes that accompany dreaming, but no support for the idea that very specific elements of dreams must have specific meanings. It is quite possible that dreams are simply the result of (or even an epiphenomenon of) other underlying processes, such as memory consolidation.
To quote a 2009 review by Hobson:
Dreaming has invited as many speculations about its function as it has triggered theories about its mechanistic source. There is an important distinction to be made between dreaming, which is a subjective, psychological state, and REM sleep, the brain state with which it is most highly correlated, especially when discussing function. Many of the functional theories for dreaming that have been advanced have assumed a single identity for the two domains of discourse, despite the fact that we can speak only of a correlation. Here I focus on the function of REM sleep and assume that dreaming is an indispensable — if sometimes misleading — subjective informant about what the brain does during REM sleep. Indeed, we may be bound to admit that dreaming itself could be an epiphenomenon without any direct effect on normal or abnormal cognition.Dreaming is most associated with REM sleep, and REM sleep has itself been associated with memory formation, processing of emotional memories, and the development of intuition (e.g., solving a problem while you sleep on it).
Regarding the possible physiological explanations for dreams, I'll quote from a 2001 review by Stickgold et al:
In contrast, since Freud proposed his theory of dream interpretation (14), there has been a frustrating dearth of scientific evidence concerning the mechanism of dream construction and its possible functions. One such function might be as part of a multilevel system of sleep-dependent learning and memory reprocessing, wherein dreams would be the conscious manifestation of these processes.
While we still don't understand whether the elements of dreams have any real psychological significance, beyond replay or manipulation of daytime cortical traces, there are good physiological reasons for dreams having the character that they do:the cognitive changes seen during REM may be the combined result of three physiological characteristics of REM: (i) the shift in neuromodulatory balance from aminergic to cholinergic, (ii) the decreased activity in DLPFC and increased activity in both the anterior cingulate cortex and amygdala (75–77), and (iii) the decreased outflow of information from hippocampus to neocortex (53). Taken together, these findings suggest that the brain in REM is tuned more for the processing of associative memories than for the simple consolidation of recent memory traces and may explain, in part, various features of REM dreams, including their bizarre, hyperassociative quality (95) and minimal incorporation of episodic memories (96, 97).
During REM, limbic forebrain structures and the amygdala are activated while both DLPFC and the locus coeruleus become less active. This presumably inhibits the ability of DLPFC to allocate attentional resources (and the dreaming brain classically pays little attention to bizarre incongruities in dreams). At the same time, the inhibition of hippocampal outflow would prevent the reactivation of episodic memories (53). Dreams would thus be constructed largely from those primarily weak neocortical associations available during REM (92). Although the process of incorporation of these weak associates is unknown, we predict that associated emotions, mediated by both the amygdala and medial orbitofrontal cortex, play an important role. Thus, the resulting dreams would appear to be not only unpredictable and bizarre but highly emotional as well.
Most research points to combinations of person, place and context cues along with visual associations of their emotional salience taken from the immediate day before (Day residue) and from units of 7 days prior. And a recent paper elaborating on the discontinuity of dreams suggests a heightened link between memories and dreams between a certain time period, although the overall association between memories on a given day and dream content is weak.
I don't know of any evidence to support the notion that you have to get REM sleep for it to matter. The best marker we have for the restorative value of sleep is in fact the amount of slow waves ("delta waves") in the EEG, which is a marker of the depth of NREM sleep. In a normal night, you spend about 80% of the time in NREM sleep, and the amount of delta waves decreases approximately exponentially across the night. Also, if you are sleep deprived, the amount of delta waves is much higher at the beginning of the night.
In addition, short naps (less than about 30 min) almost never contain REM sleep, yet they can have a restorative effect on cognitive function.
There have been some studies linking REM sleep to certain types of memory function. However, the results can be difficult to interpret, because it is very difficult to experimentally manipulate the amount of REM sleep someone gets without messing up the whole night of sleep. For example, you can wake people up whenever they enter REM sleep to try to specifically deprive them of that stage of sleep, but then any effects you see may be due to them being continually awoken! Achieving an appropriate control is challenging.
Anti-depressants strongly suppress REM sleep, and many people take them. If the restorative value of sleep were erased by anti-depressants, then we would expect to see many more side effects than we do.
It also seems counter-intuitive that only 20% of our night of sleep would "matter". What is all the other stuff for then? REM and NREM sleep very likely each have related functions, but we're not sure what they are exactly. The fact that we cycle between REM and NREM sleep is suggestive of some sort of functional importance for this temporal sequence, but we don't know what it is exactly. The issue is complicated by the fact that different mammalian species get very different amounts of REM sleep. In general, however, REM sleep decreases with age; as newborns, we spend about 50% of sleep in REM sleep. It has therefore been suggested that it may play an important role in brain development. But again, this is just a hypothesis.
In terms of simply transitioning from what we consider "sleep" to what we consider "wake", it can be very quick, on the order of hundreds of milliseconds. As most people are aware, an alarm or disturbance can wake you very quickly.
However, people experience grogginess upon first awakening (usually called "sleep inertia"), and this lasts considerably longer. On cognitive tests, people perform extraordinarily poorly if you test them immediately upon awakening -- worse even than when they are sleep deprived.
Over the course of about 2 hours, sleep inertia asymptotically dissipates.
Why sleep inertia occurs, we don't fully understand. One hypothesis is that it takes different brain regions different amounts of time to transition from sleep to wakefulness.
 So what should you do to combat it? Caffeine reduces sleep inertia. The only problem is that it takes around an hour from ingestion to reach peak levels in the bloodstream, by which time you are usually past the worst of sleep inertia anyway.
So what should you do to combat it? Caffeine reduces sleep inertia. The only problem is that it takes around an hour from ingestion to reach peak levels in the bloodstream, by which time you are usually past the worst of sleep inertia anyway.
Bright light could help for a couple of reasons. First, light has a direct alerting effect. Second, light suppresses the secretion of melatonin, which is a sleep-promoting hormone. Upon first awakening, you may (depending on the timing) still be releasing some melatonin.
A hot shower is often anecdotally recommended, presumably because it helps to more rapidly raise your core body temperature (which is at its daily minimum shortly before your usual wake time), and because it has a stimulating effect. However, one study found no effect of breakfast, a shower, and exposure to room light on sleep inertia, as compared to people who stayed in a semi-recumbent posture in bed in dim light.
Another study found caffeine and bright light to be effective, but face washing only improved subjective sleepiness and not objective performance.
It is rather concerning to think about the number of potentially dangerous activities people engage in when they have just awoken. The risk for accidents is greatly increased during that short window of time.
There are some specific brain regions that are involved in regulating sleep/wake. Specifically, there are wake-promoting populations of neurons in the brainstem and hypothalamus with ascending projections to thalamus and cortex. During wakefulness, these neurons are active, releasing wake-promoting neurotransmitters (histamine, norepinephrine, serotonin, dopamine, acetylcholine, orexin). These neurons receive input form a sleep-promoting population of neurons in the hypothalamus (in the ventrolateral/median preoptic area). The sleep-promoting population becomes more active at nighttime and also after extended wakefulness, resulting in inhibition of the wake-promoting populations.
There are some descending projections from the higher brain to these wake-promoting populations, so you can control their outputs to a certain degree, e.g., forcing yourself to stay awake for a while.
However, sleep is also regulated locally throughout the brain. During wakefulness, certain sleep-regulatory substances accumulate in the extracellular space, including adenosine, prostaglandin D_2, and cytokines. We now know that when an animal becomes very tired, local regions of cortex can fall "asleep" while the animal is still behaviorally awake. When you are struggling to stay awake, you are therefore probably also fighting against a gradually failing neuronal network.
It's a great question that's surprisingly hard to answer! Fever can be induced by chemicals called pyrogens. Many cytokines (immune-signalling molecules) are pyrogens. When you get an infection, your body releases more cytokines.
There are well established connections between cytokines and sleep. Specifically, a higher concentration of some cytokines induces sleepiness, which is why you get sleepy when you have an infection. Altered sleep during infection is thought to be part of the acute-phase response to help recovery. Interestingly, when you get insufficient sleep, your immune system function is impaired -- people who habitually sleep less than 7 h per night are ~3 times more likely to contract the common cold following exposure via nasal drops than those who habitually sleep more than 8 h per night.
 You might then surmise that since our most vivid dreams occur dreaming REM sleep (note that it is possible to have dreams in NREM sleep too, they just tend to be more mundane) we must get more REM sleep when we are sick and have a fever. Surprisingly, however, increased cytokine concentrations and fever result in less REM sleep! This may be partly due to the fact that during REM sleep, shivering is not possible due to muscle atonia, making it more difficult to efficiently thermoregulate.
You might then surmise that since our most vivid dreams occur dreaming REM sleep (note that it is possible to have dreams in NREM sleep too, they just tend to be more mundane) we must get more REM sleep when we are sick and have a fever. Surprisingly, however, increased cytokine concentrations and fever result in less REM sleep! This may be partly due to the fact that during REM sleep, shivering is not possible due to muscle atonia, making it more difficult to efficiently thermoregulate.
So what's going on? Well, sleep is often much more fragmented when we have a fever. Body temperature generally decreases during NREM sleep. It has been proposed that frequent awakenings to raise temperature may be a mechanism to prevent undue heat loss.
A plausible (but by no means verified) answer to your question is that people simply remember more dreams due to sleep fragmentation associated with some fevers. People dream every night and will report dreaming about 90% of the time if awoken from REM sleep. These dreams are typically vivid and bizarre in character. However, we don't usually remember most of these dreams because short-term memory does not function normally during sleep. You only tend to remember a dream well if you are awake for some time after it.
It's also plausible that the temperature change that is the fever is to blaim. All chemical reactions that I am aware of are affected by temperature. Some go faster when the temperature gets elevated, some go slower. Since at a fundamental level all biology reduces down to chemical reactions, it is reasonable to conclude this is the case.
The acute hormonal changes associated with nightmares are not particularly well studied. There have been some studies looking at changes in autonomic tone, including heart rate and respiration, showing that there are occasionally measurable effects of nightmares. Quoting from this review.
Most healthy individuals experiencing a nightmare (that is, individuals from a non-psychiatric sample), exhibit a moderate level of heart rate acceleration for the last three minutes prior to awakening during a nightmare REM sleep episode, while an equal proportion of healthy individuals usually manifest heart rate deceleration during non-nightmare REM sleep (Nielsen & Zadra, 2000). The EEG samples of these subjects also show cortical activation during the last two minutes of nightmare, exhibiting an amplification of the posterior alpha power observed during normal REM sleep, but also an atypical higher beta power over frontotemporal regions (Cantero, Atienza & Gomez, 1999).
 Another review has a couple of passages relevant to your question:
Another review has a couple of passages relevant to your question:
Physiologic evidence for emotional activity during rapid eye movement (REM) sleep is substantial. Autonomic system variability increases markedly in conjunction with central phasic activation, as seen especially in measures of cardiac function, respiration, and skin and muscle sympathetic nerve activity. Brain imaging, too, demonstrates increased metabolic activity in limbic and paralimbic regions during REM sleep activity similar to that seen during strong emotion in the waking state. These dramatic autonomic fluctuations globally parallel dreamed emotional activity, which is detectable throughout most dreaming when appropriate probes are employed. Some studies indicate that most dreamed emotion is negative, primarily fearful, and may conform to a surgelike structure within REM episodes. Many theorists interpret the various forms of phasic activity occurring during sleep as indicating dream-related affective activity.
One laboratory study of nightmares indicates moderate arousal—increased heart and respiration rates—during some nightmare episodes, but unexpectedly low arousal in most others. These early findings constitute the principal empirical basis for diagnostic guidelines such as the ICSD and DSM-IV, but there are serious problems with the work, such as the inclusion of psychiatric patients and patients with posttraumatic stress disorder (PTSD) in the study sample.
Recordings of heart rate and respiration rate during nightmare and non nightmare REM sleep episodes confirmed a moderate level of sympathetic arousal during nightmares. Mean heart rate for nightmare sleep was elevated (by about 6 bpm) for the 3 minutes before awakening. Mean respiration rate was only marginally higher at this time. We have recorded higher absolute and relative alpha power over primarily right posterior sites in the last 2 minutes of nightmare sleep. However, these changes might reflect processes of awakening.
The grogginess one feels upon waking up is usually called "sleep inertia". Upon awakening, people perform worse on cognitive tasks for up to 2 h afterwards, which can make it dangerous to drive. Sleep is typically broken into the following stages:
Sleep is typically broken into the following stages:
Rapid Eye Movement (REM) Sleep: During this stage, brain activity looks similar to wake. However, you have very little muscle tone, and you are usually dreaming.
Non-REM (NREM) Sleep Stages 1-3: Stages 1-3 are in progressing order of depth. It is the hardest to wake someone during the deepest NREM sleep, and the brain activity includes progressively more large amplitude slow waves the deeper into NREM sleep.
Sleep inertia tends to be worst when awakening from the deeper stages of NREM sleep. Without any disturbances, a regular night of sleep consists of an initial progression through NREM stages 1 to 3, followed by an approximately 90 minute cycle between NREM and REM sleep. Across the night, the REM sleep bouts get progressively longer, and the NREM sleep bouts get progressively shallower.
There are many spontaneous awakenings across a regular night of sleep. However, awakenings are much more likely to occur out of REM sleep or the lighter stages of NREM sleep.
You would guess, then, that when one is forced awake, they are more likely to be entering wake from a deeper stage of sleep than if they awaken spontaneously. Consequently, the sleep inertia would be more severe. This paper found that, indeed, sleep inertia was worse after forced awakenings than after self-awakenings. However, the number of participants was not really sufficient to determine whether there was a systematic difference in the sleep stage from which they awoke. Within their sample, the self-awakening subjects were actually more likely to awaken from stage 2 NREM sleep and less likely to awaken from stage 1 NREM sleep, which is the complete opposite of what you would expect. It's therefore unclear what the underlying mechanism is. My guess is that it's something fundamental about how the transition from sleep to wake is initiated, possibly associated with local sleep.
As for what local sleep is: It has recently been discovered that sleep is not necessarily a whole-brain phenomenon. Parts of the brain can be "asleep" while others are "awake".
When you spontaneously awaken in the morning, it is probable that not all of your brain is yet awake. It takes time for all of the regions of the brain to make the transition from the sleep state to the wake state. This has been proposed as a mechanism underlying sleep inertia. If you are woken up suddenly by something else (e.g., an alarm clock), less of those brain regions may be ready for making the transition from sleep to wake, which may result in more severe sleep inertia. That is a more speculative explanation, mind you, but also quite plausible.
I don't think we can get a definitive answer to this question, since controlled sleep surveys go back no further than 100 years.
Nevertheless, we do have some evidence to work with. First, there are historical records. Second, there is what we can infer from our basic physiology.
In terms of historical records, Ekirch has done some digging into how people slept in medieval times. (He has a curious book called At Day's Close if you are interested).
 In this lengthy review, he explores how people slept in the British Isles before the Industrial Revolution. Here is the most relevant quotation:
In this lengthy review, he explores how people slept in the British Isles before the Industrial Revolution. Here is the most relevant quotation:
Diaries, though heavily weighted toward Britain's upper classes, suggest not only that adults typically slept for periods of from six to eight hours but that the standard time for retiring to bed fell between nine and ten o'clock.In addition, Ekirch presents some evidence that sleep may have been divided into two chunks during the night, with some time spent awake in the middle.
Even across the 20th century, there was a shift towards later bedtimes. Certainly, we go to bed much later today than people in medieval times, but we awaken not much later, resulting in a reduction in sleep duration overall.
Regarding physiology, we know that the human circadian pacemaker is acutely sensitive to light and that artificial light in the evening delays the clock and suppresses melatonin. Both of these factors push sleep onset later.
Without artificial light (e.g., when camping), the circadian rhythm is shifted to an earlier phase and people initiate sleep and wake earlier. It's difficult to say precisely how much earlier, since that varies by individual and environmental conditions, so without detailed historical studies we are guessing to an extent.
I'll start with an essential caveat, which is that we don't have a gold standard way of defining "how much sleep an individual requires". What most studies measure is how long people habitually sleep, which is really a combination of sleep need and any other social or biological factors that affect sleep duration.
We know that there are individual variations in the amount of sleep people habitually choose to get. We also know that there are differences in the sleep homeostatic process between habitual short-sleepers and habitual long-sleepers. There was also a genetic association recently discovered between DEC2 and the amount of habitual sleep people get.

What we don't know yet is whether people who sleep less actually need less sleep (i.e., their sleep is somehow more efficient), or whether they simply are unable to sleep for as long and bear the consequences in terms of long-term impairments and health problems. Epidemiological studies consistently show worse outcomes for individuals who habitually sleep less than 6 h or more than 9 h -- however, as well as we try to control for these things, epidemiological data are possibly confounded by correlations between sleep duration and other lifestyle or health factors.
We also know that some people are more resilient to the effects of sleep deprivation than others. However, there are no studies I am aware of that show people consistently sleeping 4 hours per night and performing at a normal cognitive level.
There are many apocryphal stories told about high achievers getting by on very little sleep, and indeed there is a whole culture linking short sleep to toughness and success -- sleep is for the weak!
However, we know that sleep plays critical roles in maintaining memory, optimizing cognitive performance, pruning synapses, and managing the brain's energy balance. The idea that skimping on sleep will somehow boost function has no face validity.
It is conceivable that there is a correlation between intelligence and resilience to sleep loss or efficiency of sleep, but the data to test that hypothesis don't presently exist. In fact, the evidence we have suggests that those who sleep habitually less score worse on IQ tests.
First off, there is no answer to your question. But it's still a good question! Here's why there's no answer:
If we want to know how much sleep your body needs, we need to know what it needs sleep for. It's not to recharge energy: your body is quite capable of those processes while awake (and asleep).
A few of the current known functions of sleep: regrowth (healing), memory processing (memories are consolidated and organized).
How much sleep does your body need to heal? Well, this process still functions while awake, just slower, so technically none.
How much sleep do you need for memory processing? Who knows, there are so many questions to be asked. How many memories did you make? Were they vivid or redundant? Multiple small events or a big large one? How many other memories are associated with those events? We can't get a valid general-use answer from this function.
Complications abound: Did you get a lot of bright light? How much did you sleep the night before? Did you use any brain altering drugs (e.g. caffeine)? Did you exercise? What did you eat? How is the weather? And the biggest, who are you (weight, age, habits, genetics)?
We have no real understanding of how much your body needs, we only have data and conclusions and averages and assumptions. And we're still struggling with the big question, "Why do we need sleep?"
But all that said, here's an answer anyway: There was a time when people had no alarm clocks. Your body is built to schedule sleep around nighttime. Two main components affect this, your circadian rhythm, and your need to sleep (not the previously mentioned sleep need = duration of sleep). On a consistent daily sleep schedule, this will normalize and you will sleep for relatively the same amount of time each night, sleeping and waking up at relatively the same time. There are many factors involved that can distort this. If the schedule is not consistent, then neither will the sleep be.
In general, naps are beneficial in reducing the effects of sleep deprivation. 1-2 hours of sleep is certainly not healthy, but it is better than nothing (although see the caveat below).

For example, this study kept participants awake for 88 hours. One group had to stay awake the whole time, while the other group were allowed a 2-hour nap every 12 hours. The nap group performed vastly better in terms of cognitive performance and reaction times.
Another study kept all participants awake for 39 hours. After 14 hours awake (at 9pm), some participants were given a 2-hour nap. Those who were allowed to nap performed significantly better in terms of mood, alertness, and performance.
The other important thing to consider with naps is sleep inertia, which is the groggy feeling upon first waking up. Sleep inertia is due to the time it takes for the brain to transition from sleep to wakfulness. It is therefore most severe when awakening from a deeper stage of sleep.
Within the first few minutes of awakening from deep sleep, performance is considerably worse than after 24 hours of continuous wakefulness. Any nap longer than about 10 minutes results in sleep inertia. The effects of sleep inertia dissipate over ~1-2 h. So, if a task has to be performed within this critical window, a long nap will actually result in worse performance. Beyond that, the nap is beneficial.
Why sleep inertia happens, exactly, we're not sure. But it does take the brain time to get back up to speed after being asleep. This is why it's dangerous to do things like driving shortly after awakening.
Sleep inertia seems to be worst when awakening from the deeper stages of NREM sleep. A very short nap (less than about 15 min) results in very little sleep inertia, as you do not progress very far into sleep. However, the long-term benefits are also smaller for shorter naps. The sweet spot for a "power nap" seems to be about 10 min. There, you get some reduction in sleepiness and very little sleep inertia.
A 2-3 h sleep will take you deeper into sleep, resulting in more sleep inertia. In the long-term (i.e., more than 2 h after the nap), you are better off having had more sleep though.
Muscle atonia only occurs during REM sleep, which constitutes about 20% of the night in adults. In NREM sleep, which makes up the other 80%, muscle tone is low, but it is perfectly possible to move around. People who sleep talk and walk do so during NREM sleep. There are also usually ~20 brief awakenings per night, during which people often adjust their posture or roll over.
People do fall out of bed, it's just rare. It is presumed that during sleep we still have some sense of our orientation and position -- that would certainly have been necessary for our ancestors to successfully sleep in trees. I don't think we know exactly how that is achieved though.
Lucid dreaming is acknowledged, although there is certainly plenty of psuedoscience associated with it, so one has to tread carefully when reading about it. Good studies have been done to verify the existence of lucid dreaming and to determine its physiological correlates. In general, lucid dreaming is observed in REM sleep. However, some subtle differences in the EEG have been reported.
This is not a bad overview. The author explains how REM sleep is usually divided into phasic and tonic substates. Lucid dreaming appears to be more common during phasic REM sleep.
A recent study relevant to this question is this one. The authors report that lucid dreaming occurs in REM sleep, but some aspects of the EEG resemble wake, suggesting that lucid dreaming may be a hybrid REM/wake state.
As you probably already know, babies spend most of the day asleep. In a newborn, total daily sleep duration is around 14-17 hours, and we think it is even longer than that prior to birth.
Sleep duration decreases with age and, interestingly, so does the percentage of rapid eye movement (REM) sleep. Here's a nice graphic showing the changes with age here.
In a baby, over 50% of total sleep duration is REM sleep, whereas it's around 20% in an adult.
In an adult, REM sleep is strongly associated with dreaming. It is when our most vivid dreams occur and if you wake someone from REM sleep, they are highly likely to report dreaming. Dreams also occur in non-REM (NREM) sleep though, it must be noted.
As to whether babies consciously experience dreaming, we don't know. We certainly can't ask them, so in that sense we can't ever really know. Mind you, that hasn't stopped us concluding that other mammals very likely dream based on:
{kind=link}
However, we also don't yet have a sufficient understanding of what types of brain activation are present in a sleeping baby's brain. Any conclusive answer is impossible right now.
Of the parasomnias, sleep-talking is one of the most common. We don't know the exact mechanisms underlying most parasomnias, but they are generally thought to result from partial arousal of some brain regions, resulting in a mixture of sleep and wake states. Quoting from this review:
Parasomnias are defined as unpleasant or undesirable behavioural or experiential phenomena that occur predominantly or exclusively during sleep. They were initially thought to be a single phenomenon, often attributed to psychiatric disease. It is now clear that parasomnias are not a unitary phenomenon but rather are the manifestation of a wide variety of completely different conditions, most of which are diagnosable and treatable. The common parasomnias are another example of ‘dissociated sleep states’, representing the simultaneous admixture of wakefulness and either NREM sleep (disorders of arousal such as sleepwalking or sleep terrors) or wakefulness and REM sleep (REM sleep behaviour disorder). Parasomnias may result in striking clinical phenomena, which appear as the brain becomes reorganized across states, and are therefore apt to occur during the transition from one state to another.
In view of the large number of neural networks, neurotransmitters and other state-determining substances that must be recruited synchronously for full state declaration and the frequent transitions among states during the wake–sleep cycle, it is surprising that errors in state declaration do not occur more frequently than they do. In addition to the phenomenon of state dissociation, in which two states of being overlap or occur simultaneously, there are probably additional underlying physiological phenomena that contribute to the appearance of complex motor behaviours during sleep. These include: activation of locomotor centres during sleep, sleep inertia (a period of confusion or disorientation during the transition from sleep to wakefulness) upon arousal and sleep state instability (oscillation between wakefulness and sleep). The parasomnias, which are usually due to admixtures of states of being, along with narcolepsy, support the concept that wake and sleep are not mutually exclusive states, and that sleep is not necessarily a global brain phenomenon.
Experimental studies have demonstrated that sleep is a phenomenon that can occur locally. In other words, some brain regions can be awake while others are asleep.
Studies in humans have also shown local brain activation associated with confusional arousals.
In NREM sleep (where most parasomnias occur), the body is not paralyzed. Partial activation of motor regions may therefore result in activities such as sleep-walking and sleep-talking.
This is a very interesting question that we should
On Earth, virtually all organisms have circadian clocks and they have evolved to have periods very close to 24 h. The average period differs slightly by species and also by individual. In humans, for instance, the average period is 24.15 h.
Because the circadian period is never exactly 24 h, the clock requires some resetting each day to remain synchronized to the 24-h day. That resetting is primarily achieved by light. There are certain ganglion cells in the retina that are sensitive to light and project to the master circadian clock (in the suprachiasmatic nucleus).
The amount of resetting light can achieve each day depends on the species, the intensity of light, and timing of light exposure in the circadian cycle. Generally, it would be very difficult if not impossible for a human to entrain to a 20-h or 28-h day. In fact, some experiments (called forced desynchrony experiments) make use of this fact by forcing people to live on a non-24-h sleep cycle. Under these conditions, the circadian clock fails to entrain to the new day and instead continues to run at a period close to its intrinsic period.
In practice, people can reasonably entrain to a day length up to about 1-2 h longer or shorter than their intrinsic period. This experiment showed that room light (100 lux) is bright enough to entrain subjects to a day 1 h longer than their intrinsic period, but the entrainment is weak, resulting in people waking and sleeping at unusual times of day. Adding a couple of 45-min pulses of bright daytime light (9500 lux) results in good entrainment to the new day length.
 The Mars day is 24.6 h long, so most humans would be capable of entraining to that day length. This experiment showed that even candlelight (1.5 lux) is enough to entrain some people to the Mars day. Note that the response to light intensity is non-linear (100 lux has about half the effect of 10,000 lux).
The Mars day is 24.6 h long, so most humans would be capable of entraining to that day length. This experiment showed that even candlelight (1.5 lux) is enough to entrain some people to the Mars day. Note that the response to light intensity is non-linear (100 lux has about half the effect of 10,000 lux).
If the day length was more than 1-2 h different from 24 h, or if there was very little light, we would really struggle. Experiments in humans and animals have shown that after entrainment to a shorter or longer day, the intrinsic circadian period is slightly changed. However, this effect is generally very small. For example, this study in humans found an increase in period of 0.10 h following entrainment to a Mars day.
Over millions of years, we would possibly adapt to the new day length. We know of several gene mutations that result in unusually short or long circadian periods. For example, Clock, Period, and Cry. On Earth, such mutations are maladaptive, resulting in circadian rhythm sleep disorders, but on another planet they may be highly adaptive.
One other condition under which we may be able to adapt is if the day length corresponds to a harmonic or subharmonic of our circadian rhythm; for example, a 12-h day or a 48-h day. A wake/sleep pattern with a period of approximately 48 hours is called a bicircadian sleep pattern.
Bicircadian sleep patterns have been found to sometimes emerge under the following conditions: When people are placed in an environment free of any external time cues and allowed to self-select their schedules, they initially live on an approximately 24-25 h schedule, driven by the body's circadian rhythm. However, after a while, the sleep/wake pattern desynchronizes from the circadian rhythm. At this point, people continue to produce 24 h rhythms in body temperature and hormones, but their sleep/wake cycle takes on its own period. Why this occurs, we still don't really know, although we have some theories.
Under these conditions, sleep/wake cycles ranging from 12 h to about 70 h have been observed and the participants aren't usually aware of how far they have diverged from a 24 h day.
Interestingly, in some rare cases, the circadian and sleep/wake cycles appeared to achieve a bicircadian pattern, where subjects slept every second circadian cycle, i.e., approximately every 48 h.
Although this bicircadian pattern can emerge under these special conditions, it is not something that can ordinarily happen. Generally, your circadian rhythm can only be synchronized to day lengths close to 24 h (up to about 2 h in either direction). Attempts to artificially impose a 48 h day have been largely unsuccessful.
One last thing: It's worth noting that Earth's period has not always been 24 h. The rotation of the Earth is gradually slowing down. 500 million years ago, it is estimated to have been around 21 hours. Evidently, the historical change in solar day length has been gradual enough for evolution to keep pace with it.
This is an open question. We are quite sure that other mammals dream, for three reasons:
Moving away from mammals, there is still some debate as to whether sleep is structured the same way. As you noted, sleep appears to be somewhat different for monotremes (i.e., echidnas and the platypus). Initially it was thought that monotremes lack REM sleep, but we now think that they do have REM sleep, it just has different physiological correlates.
There is now some good evidence to suggest that birds also have separate REM and NREM sleep stages.
However, note that sleep cycles tend to occur on much shorter timescales in birds, with REM sleep bouts lasting only ~10 s. Also, many birds sleep unihemispherically (with one half of the brain at a time, like dolphins do). Whether dolphins experience dreams is not yet known -- certainly, they have very little REM sleep. It's hard to know what type of conscious experience an animal has when only half of their brain is awake!
Sleep has not yet been well studied in reptiles. Whether they have REM sleep is still an open question -- there is conflicting evidence on this point.
Some hibernating animals such as bears have evolved strategies for maintaining muscles during their dormancy. As a result, they lose very little of their muscle strength across winter.
This is thought to be achieved by bouts of muscle movement and recycling of nitrogen from urea to amino acids to produce the necessary proteins to maintain muscle.
The reason one begins to feel better towards the end of the night is due to the circadian rhythm in alertness. The body contains a circadian clock that promotes sleep during the night and wakefulness during the day. As the next day begins, that circadian wake promoting signal also begins, which partially counteracts the increasing sleepiness with time spent awake.
The same is true if people are kept awake for several days. There is an overall decline in alertness from day to day, but also a circadian rhythm in alertness within each day.
This is a big open question, so I'll start by saying that there isn't a single definitive answer.
Before we start, let's review the basics:
Circadian rhythms: A circadian rhythm is any approximately 24 h rhythm that is endogenously generated by an organism. In other words, it is not just a response to environmental (exogenous) cues, though its phase can be reset by environmental cues, allowing it to remain synchronized to the light/dark cycle. Circadian rhythms can manifest in behavior (e.g., sleep/wake), physiological outputs (e.g., hormone release), biochemical processes, or gene expression.
Rest/activity cycles: As it sounds, a rest/activity cycle is an alternation between periods of high activity and periods of low activity. While we are familiar with rest/activity cycles in complex organisms, such as humans, we can also define rest/activity for much simpler organisms (e.g., fruit flies) so long as we have some measure of "activity".
Sleep/wake cycles: Sleep is best defined in mammals as a period of: Reduced activity, and often changed posture, reduced responsiveness to environmental stimuli, ability to rapidly return to wake if a strong enough stimulus is provided, rest that is homeostatically preserved (i.e. lost sleep results in a sleep debt and impaired functioning while awake), and well-defined changes in physiological signals, including brain activity changes associated with REM and NREM sleep.
These criteria can also be applied to many other vertebrates, including zebrafish. However, it is difficult to apply these criteria to simpler organisms (e.g., those without a brain). If we are happy to accept a modified version of the last criterion then we can define sleep in many other organisms, such as C. Elegans and fruit flies. But it is still problematic to define sleep in, say, a unicellular organism.
So now that we've refreshed our memories on the terms, how can they help us? Well:
Circadian rhythms are ubiquitous
So far as we can tell, circadian rhythms exist in virtually all organisms. Circadian rhythms are highly adaptive in a world where light and temperature levels oscillate, as they allow organisms to anticipate environmental changes and make best use of their available resources. Experiments have shown that organisms with circadian gene mutations that have periods very different from 24 h are out-competed by regular (wild type) organisms. However, if both the mutant and the wild type organisms are then moved into an environment where the day length matches the period of the mutant's rhythm, the mutant out-competes the wild type.
Even in a constant environment, rhythms may be advantageous
Circadian rhythms also allow organisms to temporally separate incompatible processes. For example, photosynthesis and nitrogen fixation. So, even in an unchanging environment, there is a potential advantage to having an endogenous clock for timing processes. Certainly, we know of many ultradian (shorter than 24 h) and infradian (longer than 24 h) biological rhythms that do not appear to match the period of any particular environmental cycles.
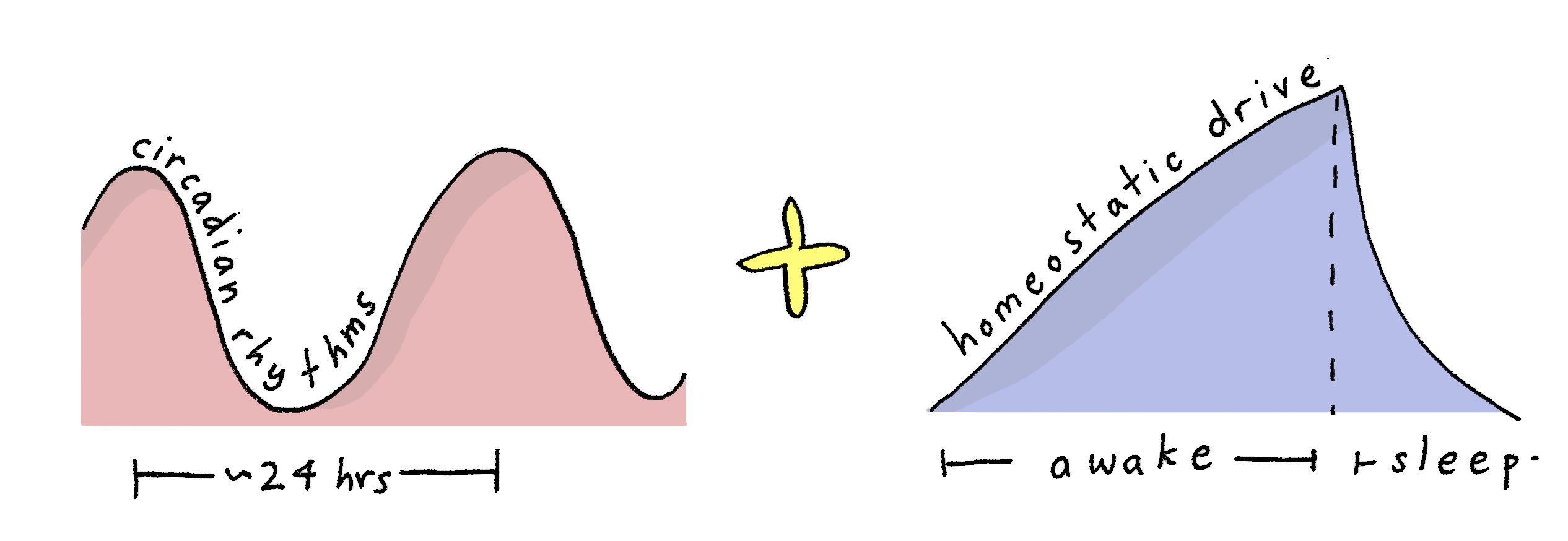
Sleep is ubiquitous
For those organisms where we can define sleep, at least. This paper is a good recent review that concludes the evidence for any animal not needing sleep is weak. Every species that has been carefully studied -- and for which we can define sleep -- appears to need to sleep.
As noted above, however, sleep is a difficult term to apply to very simple organisms. Nevertheless, it is clear that once you have a circadian clock, you gain the ability to optimally time your physiological processes across the day. In most organisms, this gives rise to rest/activity cycles, where the active phase is the time of day when it is most advantageous to be interacting with the environment, e.g., seeking food or a mate. It is plausible that species subsequently evolved adaptions to make better use of the rest phase of the cycle, i.e., performing processes that increase the efficiency of processes during the active phase. The rest phase would then be anticipated to take on many of the features of sleep, including homeostatic regulation.
Sleep and circadian rhythms are different but related
While all species that sleep have circadian rhythms, not all species sleep once per day. For instance, most mammals sleep in multiple bouts per 24 h -- they are what we call polyphasic. In some species, the sleep/wake cycle may be much more rapid than the circadian rhythm, suggesting that sleep/wake cycles are interacting with, but functionally independent from, circadian rhythms. For example, the tree shrew has a sleep/wake cycle of ~15 min. Due to its very high metabolic rate, it cannot remain asleep for long periods of time without starving. The fact that it bothers to sleep at all suggests some intrinsic benefit to the sleep/wake cycle per se. A similar argument can be made for cetaceans (such as dolphins) who sleep with one half of their brain at a time.
Different species tend to take their sleep bouts at different times of day. Nocturnal animals are more night-active, sleeping more during the light phase. Diurnal animals are more day-active, sleeping more during the dark phase.
However, a few species (including some primates) appear to be cathemeral, meaning they are equally well adapted for being active during both the light and the dark phase. These species also suggest that there is some intrinsic value to sleep/wake cycles.
 Some species live without a light/dark schedule
Some species live without a light/dark schedule
We can gain some insight from looking to species who live without a light/dark cycle. It turns out many such species still make use of their circadian rhythms, although others (such as cave salamanders) appear to lose their rhythms.
Here is a pertinent quote from a review on the topic:
One way to demonstrate that a character is adaptive is to look for loss or relaxation of this trait in environments lacking diel rhythmicity, where it has no apparent advantage (Horton 2001,Willmer et al. 2000). Subterranean mole rats (Spalax ehrenbergi) that live in constant darkness are predominantly diurnal during winter and predominantly nocturnal during summer (Kushnirov et al. 1998). Brazilian cave catfishes (Pimelodella kronei, P. transitoria, and Trichomycterus sp.) showed some degree of rhythmicity (circadian, ultradian, and/or infradian) (Trajano & MennaBarreto 1995, 1996). Most cave-dwelling millipedes (Glyphiulus cavernicplu sulu, Cambalidae, Spirostreptida) that occupy the deeper recesses of a cave show circadian rhythmicity (Koilraj et al. 2000). The hypogean loach (Nemacheilus evezard), shows a circadian rhythm of body temperature, with individually varying periods (Pati 2001). Other species, such as the European blind cave salamander (Proteus anguinus), have lost their circadian rhythmicity (Hervant et al. 2000). It has been hypothesized that the retention of some rhythmic component reflects the importance of maintaining internal temporal order or the ability to measure seasonal changes in photoperiod (Goldman et al. 1997, Horton 2001).
The problem with this approach is that these species still evolved on Earth from ancestors that did have circadian rhythms, so their evolution is still shaped by the fact that Earth has light/dark cycles.
Sleep/wake cycles may be an intrinsic property of neuronal networks
We know that sleep plays many important roles for the brain, including memory consolidation, memory balance, and synaptic pruning. We now also have evidence that sleep can occur locally within a neural network without the whole brain being asleep and that sleep/wake cycles may be a fundamental property of any neuronal assembly. When neurons are active for long periods of time, they release molecules into the extracellular space that induce a sleep-like state, leading to sleep/wake cycles.
So: Is sleep an evolutionary byproduct of the Earth's day/night cycle?
Overall, it seems that sleep serves many important functions aside from circadian rhythms. However, it is impossible to answer whether these functions emerged only because of the prior existence of a light/dark cycle and the consequent evolution of circadian rhythms and rest/activity cycles.
 Unihemispheric sleep is sleeping with only one half of their brain at a time. Cetaceans sleep unihemispherically, which allows them to continue monitoring their environment -- and of course breathing -- during the night. Manatees also sleep unihemispherically, meaning they evolved this state independently. (As an aside, there is evidence of unihemipsheric sleep in birds and reptiles, so unihemispheric sleep may even predate bihemispheric sleep, as strange as that seems!)
Unihemispheric sleep is sleeping with only one half of their brain at a time. Cetaceans sleep unihemispherically, which allows them to continue monitoring their environment -- and of course breathing -- during the night. Manatees also sleep unihemispherically, meaning they evolved this state independently. (As an aside, there is evidence of unihemipsheric sleep in birds and reptiles, so unihemispheric sleep may even predate bihemispheric sleep, as strange as that seems!)Now, true seals (phocidae) don't sleep unihemispherically, yet they spend a lot of time in the water. They get around this issue by holding their breath for several minutes at a time while they sleep in the water, periodically surfacing to hyperventilate. The same is true of several other marine mammals, include the walrus and the hippopotamus.
Interestingly, fur seals seem to have adopted a different strategy. When on land, they sleep bihemispherically, like all land mammals. However, when they are in the water, they switch to sleeping unihemispherically!
It depends somewhat on what medication was used for anesthetization, but most of them produce a brain state that is distinct from sleep. I won't comment on whether a person will subjectively experience a feeling of being rested (even though most people don't report feeling rested), but the important thing is again that being anesthetized is not the same as sleeping.
The states of sleep and anesthesia are physiologically different, so we wouldn't necessarily expect one to be able to exactly substitute for the other. However there are many interactions. Anesthesia affects many of the systems that regulate sleep, and many anesthetics actually achieve their actions by targeting those systems.
Sleep need is generally understood in terms of what is called sleep homeostasis. The longer you are awake, the more your sleep homeostatic pressure increases, and the longer you are asleep, the more it decreases. We now know that the sleep homeostat probably represents the accumulation and clearance of certain sleep regulatory molecules in the brain.

We still don't know exactly how anesthesia affects the sleep homeostat, but there have been some studies. This 2004 review says:
Work in rats suggests that during prolonged anesthesia, sleep need does not accrue, and that recovery from sleep deprivation can occur during anesthesia. Moreover, both circadian rhythmicity and sleep deprivation clearly alter anesthetic action, indicating a link between factors known to regulate sleep and anesthesia. Little is known about how the anesthetized state might modulate the mechanisms governing sleep homeostasis. Anesthetics may act either directly, by reversing the buildup of sleep ‘debt’ in the brain, or indirectly by preventing normal wake-associated processes from doing the same.
The results to date suggest that different anesthetics have different effects on sleep homeostasis. Recovery from sleep deprivation seems to occur under propofol. Sevoflurane seems to address the need for NREM sleep, but not the need for REM sleep, and the same may be true of isoflurane.
However, all of these studies have so far been restricted to rats, and they haven't looked at the effects on waking cognitive function, only the effects on sleep need and other sleep markers. I also don't know of any studies to look at the effects of anesthetics on sleep homeostasis in humans.
The times at which you feel sleepy and alert each day are largely determined by your circadian rhythm. The timing of your circadian rhythm is primarily determined by your light/dark exposure pattern. So, whether you are trying to adjust your sleep/wake schedule, or trying to adapt to a new timezone, modifying your light exposure pattern is the best way to do it.
Now, to understand how to use light to change the timing of the circadian rhythm, you have to understand phase resetting. Basically, your body contains a clock that endogenously generates a rhythm with a period close to but not exactly 24 h. If you were put into complete isolation in darkness, you would continue to wake and sleep on an approximately 24 h schedule. But it's important to note that your clock's intrinsic period is not exactly 24 h, meaning you would gradually drift out of sync with the outside world under these conditions.
The reason most of us do remain entrained (i.e., synchronized) to the 24 h day is because our clock is reset a little each day by light to maintain a 24 h period. We each have a slightly different intrinsic period. The average for the human population is 24.15 h, but everybody is a little different. Some people have intrinsic periods a little shorter than 24 h and some people have intrinsic periods a little longer than 24 h. Different people therefore require different amounts of daily resetting by light to remain entrained to a 24 h schedule.
Light has different resetting effects on the circadian clock, depending on the time in the cycle. This is sometimes described in terms of a phase response curve. Light can either advance the clock (i.e., temporarily speed it up), or delay the clock (i.e., temporarily slow it down).
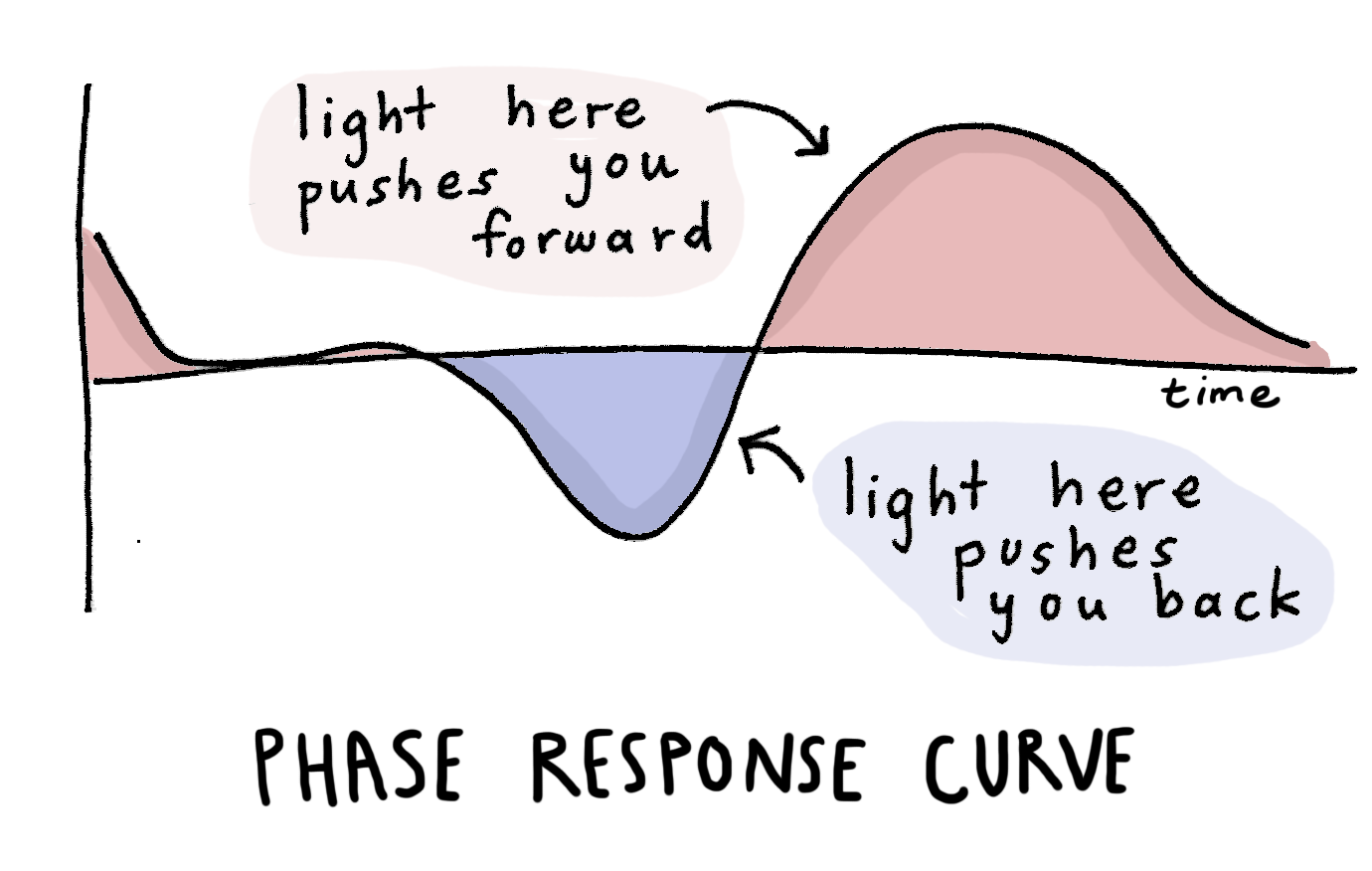
Light in your biological morning / late night (i.e., the time around when you would normally wake up) tends to advance the clock. Light in the biological evening / early night (i.e., the time around when you would normally go to bed) tends to delay the clock. [Note that these times are relative to your rhythm. If you habitually wake up at 4pm, then that may be your biological morning!]
If you wanted to shift your schedule earlier, you would need to phase advance your circadian clock. This can be achieved by doing two things: (1) Increasing your light exposure in the biological morning, e.g., going for a walk outside shortly after awakening or (2) Decreasing your light exposure in the hour or so before bed, e.g., not using a computer, keeping the light dim.
Together, these will achieve a net phase advance of the rhythm, shifting it earlier each day. Decreasing light exposure in the hour before bed will also assist in getting to sleep more quickly, because: (i) light has an alerting effect, and (ii) light exposure tells the pineal gland to stop secreting melatonin, which is a hormone that helps you to get to sleep.
Keep in mind that the circadian rhythm can only shift by so much each day, so it can take many days to move from one schedule to another. This is why jet-lag occurs, and it is also why people face problems on a Monday morning after staying up late on the weekend (a phenomenon sometimes called social jet-lag).
As an aside, I mentioned above that everyone has a slightly different intrinsic circadian period. To achieve entrainment to the 24 h day, different people therefore require different amounts of net advance or delay each day, and therefore different patterns of light exposure. For this reason, your intrinsic circadian period partly determines how your sleep/wake cycle will typically be timed relative to the natural light/dark cycle. People with longer intrinsic periods tend to be evening-types, whereas people with shorter intrinsic periods tend to be morning-types. In addition to circadian period (which you cannot control), there are many other factors that affect sleep/wake timing, including when you choose to get light each day (which you can control).
Regarding the program f.lux, it essentially reduces the blue component of the light coming from your screen after sunset. This reduces the delaying effects of light, because the circadian systems is particularly sensitive to bluer light. It doesn't eliminate the effect of light altogether, but it does help. I have been using it lately too!
 Melatonin does a couple of things.
Melatonin does a couple of things.
First, it can help you to get to sleep. In this respect, it is most effective during the biological daytime, i.e., when you would not be naturally releasing melatonin. If you take it at night and you are in dim light so your body is already producing melatonin, it has little effect. Oral doses are fine; they are absorbed fairly quickly (usually reaching peak concentrations in less than an hour). But melatonin is also cleared from the body fairly quickly (half-life is around 1-2 h). A lot of over-the-counter tablets are quite large doses, but above a certain amount it doesn't have any stronger effect (see here and here if you're interested).
Melatonin also has a phase resetting effect on the circadian clock, which is why it is also sometimes recommended for jet-lag. The phase resetting is considerably weaker than that caused by light, and the response is roughly opposite to that of light: melatonin doses in the biological morning cause phase delay and melatonin doses in the evening cause phase advance.
You can be more efficient in phase resetting your rhythm through correctly timing light exposure, and you can begin this process before you begin traveling. But ultimately, you have to shift your rhythm, and that takes time. There is some evidence that meal timing can shift the timing of circadian rhythms in other species, possibly by changing the timing of circadian clocks in other organs (since there are circadian clocks in almost every cell in the body).
That depends entirely on what you are trying to achieve. As I mentioned, the timing of your circadian clock is primarily determined by light. In terms of phase resetting, it doesn't care a whole lot whether you are lying awake or asleep in the dark. But it cares a whole lot if you turn the light on during the night. A nap during the day can help to alleviate fatigue, but it may also make it more difficult to get to sleep at night. This would probably be a big issue if you were trying to shift your schedule earlier each day. But if your goal was to shift your schedule later each day, then it may help you to stay up longer that night.
Alcohol causes problems with the placement and duration of REM stages, causes disruptions in sleep maintenance, as well as problems with SWS stages. It isn't the same for everyone, and it actually depends on how much alcohol a person has had.

Sleep architecture just means the order and duration of the sleep stages. Here is a typical night's sleep (however note that Stage 3 and 4 are now combined into Stage 3; There is no such thing as Stage 4 anymore). Alcohol makes it more likely that you will have longer REM stages earlier in the night, but it also makes it more likely that you will wake up directly from REM instead of going into Stage 1 before waking. It makes you have more brief awakenings from all stages of sleep, and decreases the amount of time you spend in Stage 3 sleep (which despite what many people believe, is incredible important for body restoration).
Regardless of whether you pass out or whether you fall asleep intentionally; alcohol, irrespective of quantity, changes sleep architecture. The problem is that there is a lot of disagreement about what the effects are and at what dosing. Having one drink, and then going to bed 3 hours later should have very minimal impact on sleep, although some research shows that it can actually alter total sleep time. There are too many variables to completely describe here, but it also matters if the person is a chronic drinker or not. Consecutive nights of sleep after drinking will be different than a single night of sleep after drinking.
There are some studies that show that in chronic alcohol users sleep architecture somewhat returns to normal (not completely) after a while. However, more recent research using newer technologies as well as measuring other metrics not measured before has shown that it's probably not as "normal" as we once thought, but it isn't certainly different than someone who rarely drinks.
Don't forget in all of this that your body is processing alcohol all the time (at a rate of around 10% per hour), so it follows what's called a blood alcohol concentration (or BAC) curve, that changes how it affects your body and brain over time. There's an ascending limb of this curve, while your BAC is still rising, and a descending limb, as your BAC is declining.
Alcohol tends to have a mild stimulating effect early in the ascending limb, then an increasingly sedating effect along the curve.
There's some evidence that once the sedating effect wears off, however (i.e. once you sober up), there is a rebound effect in the brain as the GABA receptors, enhanced by the effects of alcohol, are slow to recover. In other words, there's some evidence that once the effects of alcohol wear off you're more likely to wake up, even if you really need more sleep. Here is a great resource for more on this topic.
{kind=link}
It's called rheum and is made of water, mucin (large proteins basically), skin cells and dust (mostly).
Sleep debt turns out to be more cumulative than we once thought. A lot of early experimentation in sleep research involved completely stopping people from sleeping for some length of time (one night or several) and then letting them recover. In those instances, recovery seems to be achieved fairly quickly (within 2-3 nights).
More recently, people have looked at what happens when you lose a little sleep each night, as people tend to do in the real world. The results are worrying. Under those conditions, sleep debt builds up cumulatively over a long timescale and takes a similarly long time to recover.
In one key study people were given 8, 6, or 4 hours of sleep per night for 2 weeks. Decrements in cognitive performance (e.g., reaction time) continued to build almost linearly across the 2 weeks. Performance after 2 weeks of 6 hours time in bed per night was equivalent to being awake for 24 hours (which is about equivalent to a blood alcohol concentration of 0.10%). Performance after 2 weeks of 4 hours time in bed per night was equivalent to being awake for 48-72 hours.
 One study found that 1 night of 10 hours time in bed was insufficient to reverse the effects of 5 nights with 4 hours time in bed. Other recent data suggest that it takes at least a week to fully recover from 2-3 weeks of chronic sleep restriction. No studies have looked at what happens for chronic sleep restriction on timescales longer than that, but it probably isn't good.
One study found that 1 night of 10 hours time in bed was insufficient to reverse the effects of 5 nights with 4 hours time in bed. Other recent data suggest that it takes at least a week to fully recover from 2-3 weeks of chronic sleep restriction. No studies have looked at what happens for chronic sleep restriction on timescales longer than that, but it probably isn't good.
The effects of chronic sleep restriction are also insidious. After a few days of reduced sleep, people no longer report becoming more fatigued, although their objective performance continues to decline.
Regarding how long people can sleep, it was shown in one study that if healthy young adults are allowed 14 hours of time in bed each night for 2 weeks, they initially sleep for almost all of the allowed time. It takes about a week before average sleep durations settle down to about 8.5 h per night. This suggests that many people carry a "sleep debt" that can be expressed over many days if given the opportunity.
Are the effects completely reversible? That is a question we have not yet been able to answer. What we can say based on current evidence is the following:
In longitudinal studies, people who sleep less than 6 hours per night have poor long-term health outcomes compared to those who sleep 7-8 hours per night. This includes increased risk of obesity, cardiovascular disease, diabetes, and all-cause mortality.
In controlled laboratory studies, when people are given insufficient sleep each night for 2-4 weeks, adverse effects on cognitive performance, glucose metabolism, and immune function continue to accrue across the study time period. After these 2-4 weeks, it appears to take at least a week to recover normal functions.
So there is definitely an effect of sleep history on relatively long timescales. Moreover, if you are consistently getting insufficient sleep, one night (or even a long weekend) is not enough to bring you back to baseline.
Whether these effects continue on even longer timescales, as you are asking about, is a question of great significance (since it applies to a large portion of the population), but it is exceedingly difficult to answer. It is neither feasible nor ethical to restrict people of sleep for months to years. The only real way to look for the effects is to longitudinally study people who decide to change their sleep habits over time. It is then challenging to find appropriate controls, since changes in sleep habits are likely associated with other lifestyle changes, so if an effect is observed, it would be difficult to know how to attribute it. Right now, I don't think the necessary data exist.
 There are several popular science articles online that purport to answer this question, but I am quite sure that the answer is: we don't know for sure. Some individuals also anecdotally claim to have sneezed during sleep or observed somebody sneezing during sleep, but without recording somebody in the laboratory it is impossible to verify whether the person was truly in sleep when it occurred.
There are several popular science articles online that purport to answer this question, but I am quite sure that the answer is: we don't know for sure. Some individuals also anecdotally claim to have sneezed during sleep or observed somebody sneezing during sleep, but without recording somebody in the laboratory it is impossible to verify whether the person was truly in sleep when it occurred.
There are reports of individuals with intractable sneezing who reportedly ceased sneezing during sleep. These at least suggest that the sneezing reflex is attenuated during sleep.
The closest I can find to an appropriate study is this one, in which fluid was infused into the pharynx of sleeping newborn piglets. The authors reported that the piglets would sometimes "cough or sneeze" in response. So, with the caveat that it's a newborn piglet and not an adult human, it suggests that sneezing is at least possible during sleep given an appropriate stimulus.
As to why sneezing is very rare during sleep, the brain is less responsive to all environmental stimuli (e.g., noise, pain, etc.) during sleep. The level of stimulus required to elicit a sneeze would therefore likely be higher during sleep.
It's a well evolved trait. Animals are either nocturnal (awake at night) or diurnal (awake during the day, like us). Humans evolved to be night sleepers. The suprachiasmatic nucleus, or SCN, is the body’s master clock and provides the circadian drive to the our sleep systems. Special cells in the eyes called ipRGCs provide light input directly to the SCN. (This part of the brain is harder to fool than you think. Individuals who work night shifts suffer from mood and weight issues that day-shift workers don't have, in spite of modern lighting.)
Light has a direct alerting effect on most diurnal animals, due to the retinal input to the hypothalamus. This input drives the lower-brain systems that control our sleep and wake. This is also the reason that people tend to get sleepy in a darker environment (e.g., a dark classroom). You actually observe the opposite effect in most nocturnal animals -- they will immediately become less active and more sleepy if you put them in a brighter environment!
One of the ways in which the effects of light are mediated in humans is via the hormone melatonin. Ordinarily, the suprachiasmatic nucleus tells the pineal gland to secrete melatonin during the night. This happens with a circadian rhythm that doesn't require a light/dark cycle, i.e., if you put someone in constant darkness, they will continue to release melatonin during the night but not during the day.
Light exposure at night tells the pineal gland to immediately stop secreting melatonin. Without melatonin circulating, it is harder to get to sleep and stay asleep.
In addition, turning light off at night reduces sensory input to the cortex, which likely helps you to 'switch off' and get to sleep.
The relationship between sleep and headaches is complex. Headaches have been associated with both reduced and extended sleep. The physiological mechanism by which sleep deprivation induces headaches is still not known.
We do know that sleep has effects on both the brain and vascular function as a whole, which could certainly contribute to headaches. Additionally, prolonged wakefulness can lead to eye strain or light sensitivity, so headaches following sleep loss could be as much to do with light exposure as the sleep deprivation itself.
The brain contains an ascending arousal system in the brainstem and hypothalamus. The clusters of neurons (nuclei) that make up this system secrete wake-promoting neurotransmitters and project diffusely to the higher brain. These neurotransmitters include:
During sleep deprivation, expression of these wake-promoting neurotransmitters generally increases. This is presumably necessary to overcome the increasing pressure to sleep. Some specific findings on this point include:
Interestingly, acute sleep deprivation is a potent anti-depressant, perhaps due to the increase in monoaminergic neurotransmitter release. It's of course not an effective long-term anti-depressant, however, as people tend to have even worse mood after continued insufficient sleep.