Why 100 % O2 Is A Dive Site Necessity
by
Larry "Harris" Taylor, Ph.D.
This
material is copyrighted and the author retains all rights.
This article is made available as a service to the diving community by the
author and may be distributed for any non-commercial or Not-For-Profit use.
All rights reserved.
This
article is based
on material presented in the author’s DAN O2 Provider Class.
Go To: Home About "Harris" Articles Slides War Stories Editorials Links Fini
The
ability of oxygen to relieve the symptoms of decompression illness (Caisson's
Disease) has been known since the mid 1800's. Much of this early work is
summarized in Paul Bert's classic work, Barometric Pressure, written in 1877.
The use of oxygen by recreational divers as a first-aid measure has been
promoted for more than three decades. A training organization, DAN, was founded
in the US with a primary goal of getting the message of on-site O2
delivery to the recreational community. Yet, despite all the effort of diving
educators, there is still a major lack of understanding in recreational divers
for the need to deliver the highest possible O2 concentration to the
victim of a diving accident. Perhaps, this stems from an unfamiliarity of the
reason behind the hyperbaric medical community's recommendation that those
suffering from a diving malady be treated with100% O2.
A
decompression event can be envisioned primarily as a "bubble
disorder." A bubble of inert (not
used in body metabolism, so it accumulates) gas has formed within the body. This
bubble may impede nerve impulses, block circulation, or trigger a variety of
cellular processes designed to cope with foreign-to-the-body molecular invaders.
The symptoms seen in the victim will depend on how much gas has formed bubbles
and where these bubbles are located. Our mission, at the first responder level,
is to reduce, as much as possible, the magnitude of this "bubble
trouble." An understanding of
simple gas dynamics gives us the rationale for the need to deliver 100%
oxygen
From
a standpoint of "molecular psychology," gas molecules tend to ignore
the presence of other types of gas and focus only on their own kind. Each
element or compound present in the gaseous state will act independently, as if
they were alone. If a gas-permeable barrier (like a cell wall or the interface
between a liquid and a gas) is introduced into the system, then each type of gas
will independently try, in terms of "molecular sociology," to acquire
the same population of their type of molecule on both sides of this barrier. Gas
molecules will freely move in both directions across the barrier, but the net
movement into or out of the gas pocket will be directed towards making the
concentration the same on the inside and outside of the bubble. The movement of
each gas type will be primarily dictated by the DIFFERENCE in
concentrations between inside and outside of the gas pocket for each type of gas
present within the bubble.
So,
let's consider a nitrogen (or any inert gas in the breathing mix) bubble inside
a diver. In decompression sickness, the gas will be nearly all inert gas derived
from the breathing mix that has percolated out of tissues. In an air embolism,
the bubble initially will be about 80% nitrogen, but since oxygen can be used in
cellular processes, the oxygen diffuses away and is rapidly consumed by
metabolic reactions. So, for sake of argument, all DCI events can be considered
primarily an inert gas bubble trouble event.
Since
the body's chemical machinery cannot utilize the inert gas, it just accumulates
and interferes. If we want to "denitrogenate" (get rid of the
offending inert gas bubble) the body, we must introduce an environment that
contains NO NITROGEN (or whatever gas was used as the inert gas in the
breathing mix). We could use ANY gas that was NOT nitrogen. Anything! Carbon
monoxide, hydrogen cyanide, argon, or methane would do the job of removing
nitrogen from the bubble. Of course, the gasses just mentioned are toxic to
life, and, if, unused by the body, would themselves, accumulate in the bubble.
So, although they would "denitrogenate," it is probably best, because
of their toxicity, that we do not use them. Instead, consider oxygen.
If
we could surround the offending nitrogen bubble with a ZERO nitrogen
concentration atmosphere by introducing a 100% oxygen environment, we give rise
to the scenario shown in figure 1.
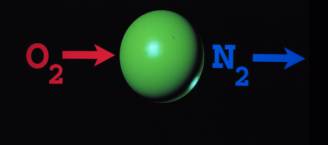
Figure
1. "Denitrogenation" Scheme
In terms of "molecular sociology:" when we surround the nitrogen bubble with 100 % O2
1.There is no N2 outside the bubble, so N2 moves out in an attempt to equalize concentrations on the inside and outside of the bubble.
2
There is
no O2 inside the bubble, so O2 moves into the bubble.
Eventually, from this simplistic static point of view (reality is a bit more complicated) with initial influx of O2 slightly enlarging the bubble before shrinkage becomes noticeable during a constantly changing dynamic process driven by changes in gas concentrations, the N2 moves outside the bubble and is transported away by circulation and the O2 moves inside. So, the bubble, near the end stages of this scenario is composed primarily of O2. But, the body metabolism uses O2. Thus, the bubble disappears as the surrounding cells consume the oxygen diffusing out of the bubble.
Why
all the hype about 100%? Does it
work?
Examine
the cat brain shown in figure 2.
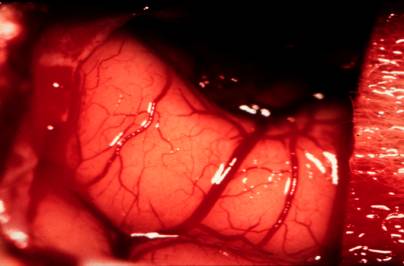
Figure
2. An exposed cat brain
Pay
particular attention to the red areas in the brain. They are blood vessels. From
the simplistic point of view of a biochemist, "Blood is life!" So,
wherever there is red, there is blood. Cells are receiving nutrients and oxygen.
Waste products like CO2 are being removed. Now, let's embolize the
cat brain with a bolus of air injected into the carotid artery. This is shown
below in figure 3.
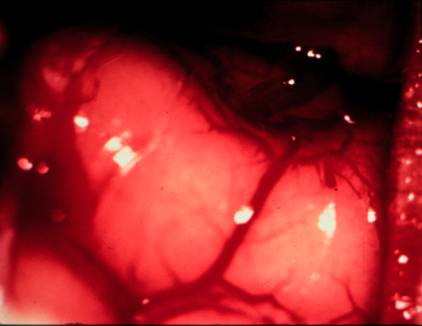
Figure
3. Cat brain following injection of air into the carotid artery.
Notice
the lack of red in the brain region. The blood vessels are blocked by air. There
is a "vapor lock" in the brain's circulation and cells not receiving
nutrients are beginning to die from lack of necessary fuel and oxidizer while
drowning in their own waste. Within minutes, neural tissue will start to die and
once dead, most likely will never function again.
Now,
let's put the cat on 100 % O2.
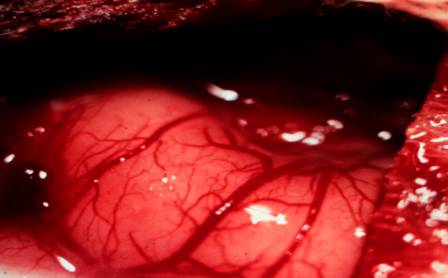
Figure
4. Cat brain with circulation restored by oxygen administration.
It
is clear that O2 shrinks bubbles. This process has been described as
miraculous!
Microscopic
examination (see references, below) of animal tissue that has been rapidly
decompressed to generate a massive bubble population revealed that in the
presence of a 100% O2 atmosphere the bubbles shrink and disappear
from view in about 2 hours. This "denitrogenation" is something YOU
CAN DO on the dive site and the reason why delivery of 100% O2 is
so emphasized in diving first-aid management classes.
So,
why all of the hype about demand valves?
The rate of gas movement out of the bubble is primarily determined by concentration of inert gas on the outside of the bubble. ANY NITROGEN IN THE BREATHING MIX WILL SLOW DOWN THE REMOVAL OF NITROGEN FROM THE BODY! (Remember, this process is driven by DIFFERENCE in concentration, the greater the difference between inside and outside of the bubble, the more rapidly the nitrogen will move outward) The best possible first responder scenario is for the patient to breathe 100% O2 (0 % N2.). This promotes "denitrogenation."
Most
oxygen delivery equipment (see Oxygen Delivery
Devices ) is meant to deliver lower than 100% O2. This is because
most O2 delivery equipment is DESIGNED to treat shock-associated
hypoxia that occurs from trauma or disease. This is NOT the same as using O2
to "denitrogenate!"
In
diving, since our mission is primarily to "denitrogenate," our O2
delivery devices MUST address this need. That is why the demand inhalator (only
device available that delivers 100% O2 to a breathing patient while
meeting the patient's full respiratory needs) is considered the best
device for treating a decompression illness incident and should be the delivery
device of choice in the on-site first responder management of a dive malady.
On
the Site
Remember
our primary task on the site in the management of a diving malady is to "denitogenate"
the body of the diving accident victim. Thus we should seek to deliver the
highest possible concentration of O2
available and to use it until the gas supply is exhausted or
relieved by a higher medical authority. If a demand system is NOT available, use
whatever is the highest possible concentration delivery device on the scene.
Bottom
Line:
Our
mission ("denitrogenation" vs. shock associated hypoxia) in a diving
accident is different from that of most every other use of oxygen administration
by first responders. Since our mission is different, we must use the tools
designed specifically for our task.
AND
With
respect to "denirogenation," nothing works better for a breathing
patient than a demand system. (The DAN MTV system is preferred for a
non-breathing patient.) This is why our dive accident management equipment
should include a demand delivery system and a supply of USP Oxygen sufficient to
supply a diving accident victim for the time it takes to get assistance from the
emergency medical community.
Acknowledgement:
The
cat brain slides were a kind gift from Lee Somers of the University of Michigan.
References
On Bubble Shrinkage
Hydlegarrd, O. & Madsen, J. Influence Of Helox, Oxygen and N2O-O2 Breathing On N2 Bubbles In Adipose Tissue, Und. Biomed. Res.16(3), 1989, 183-193.
Hyldegarrd, O. Moller, M. & Madsen, J. Effect of He-O2, O2, and N20-O2 Breathing On Injected Bubbles In Spinal White Matter, Und. Biomed. Res. 18,(5-6), 1991, 361-371
Hyldegarrd, O. Moller, M. & Madsen, J. Protective Effect Of Oxygen And Heliox Breathing During Development Of Spinal Decompression Sickness, Und. Biomed. Res. 21,(2), 1994, 115-128.
Hydlegarrd, O. & Madsen, J, Effect Of Air, Heliox, And Oxygen Breathing On Air Bubbles In Aqueous Tissues In The Rat, Und. Biomed. Res. 21(4), 1994, 423-424.
Go To: Home About "Harris" Articles Slides War Stories Editorials Links Fini
Article History
This article was originally written at a time (mid-1980's) when some in the recreational dive community was resisting the suggestion that dive site oxygen was of potential use in treating a dive accident malady. One major training agency even stated that demand oxygen devices were too complicated for diver's to use. (The fact that the scuba second stage regulator was a demand device was, of course, irrelevant). The article was expanded in the mid-90's with the publication of Hydlegarrd's bubble measuring articles.
About
the Author:
Larry
"Harris" Taylor, Ph.D. is a biochemist and Diving Safety Coordinator
at the University of Michigan. He has authored more than 200 scuba related
articles. His personal dive library (See Alert Diver, Mar/Apr. 1997, p. 54) is
considered by one of the best sources of information in North America.
All rights reserved.
Use of these articles for personal or organizational profit is specifically denied.
These articles may be used for not-for-profit diving education