Mouth Geography...Or,
Sleep Apnea and Linguistics?
William E. Arlinghaus
The University of MIchigan, A.B. Theoretical Linguistics
Broadly
viewed, the human mouth is a cave. Stalactite upper
incisors fit neatly into stalagmite lowers. A salivary river
keeps the cave moist and feeds a host of small organisms that populate
this cave. The uvula, a skin flap at the back of the mouth, hangs
down into the entry to the
air passage into the body. (If you wish to read about the biology
of the uvula, please check out any number of other sites.) The
uvula has a linguistic function in the formation of some consonants.
In
some individuals, when the uvula flops against the back of the mouth
cavity during sleep, a blockage of air flow occurs and the supply of
oxygen is cut for a few instants. This problem can apparently be
more than mere snoring; it can be a serious medical issue called sleep
apnea. Thus, the uvula serves as a sort of a dam to the flow of
air.
One way to improve flow is to remove the dam. Indeed, uvular
surgery appears to be one solution to serious sleep apnea. Unlike
the concrete man-made dam, the uvula is living tissue including muscle
fiber. Thus, it
seems natural to wonder if there might be a way to "train" the tissue
to stay out of the dam-like position: to divert the dam's action
on the flow rather than the flow's action around or over the dam.
Language trains parts of the mouth. From English, the tongue
learns to take a position to say "th". From Zulu, it learns
various clicks to supplement vocal chord noise. There are
numerous interesting sounds that come from the myriad human languages
of the world. Indeed, there are languages that employ the "uvular
trill" as supplementary to vocal chord sounds. Most or some
dialects of French, German, Dutch, Italian, and Swedish employ the
uvular trill. Thus, several
research questions of possible interest emerge:
1. Do individuals who use the "uvular trill" as part of their
language pattern on a regular basis have better "trained" uvular muscle
fibers than
do others?
2. Do language groups using uvular trills have a lower (higher)
incidence of sleep apnea than do language groups not employing the
uvular trill?
3. Depending on the answer to 2, might training of the uvular
muscles,
through the systematic linguistic study and practice of phonetics,
divert the damming effect of the uvula and relieve at least some sleep
apnea issues?
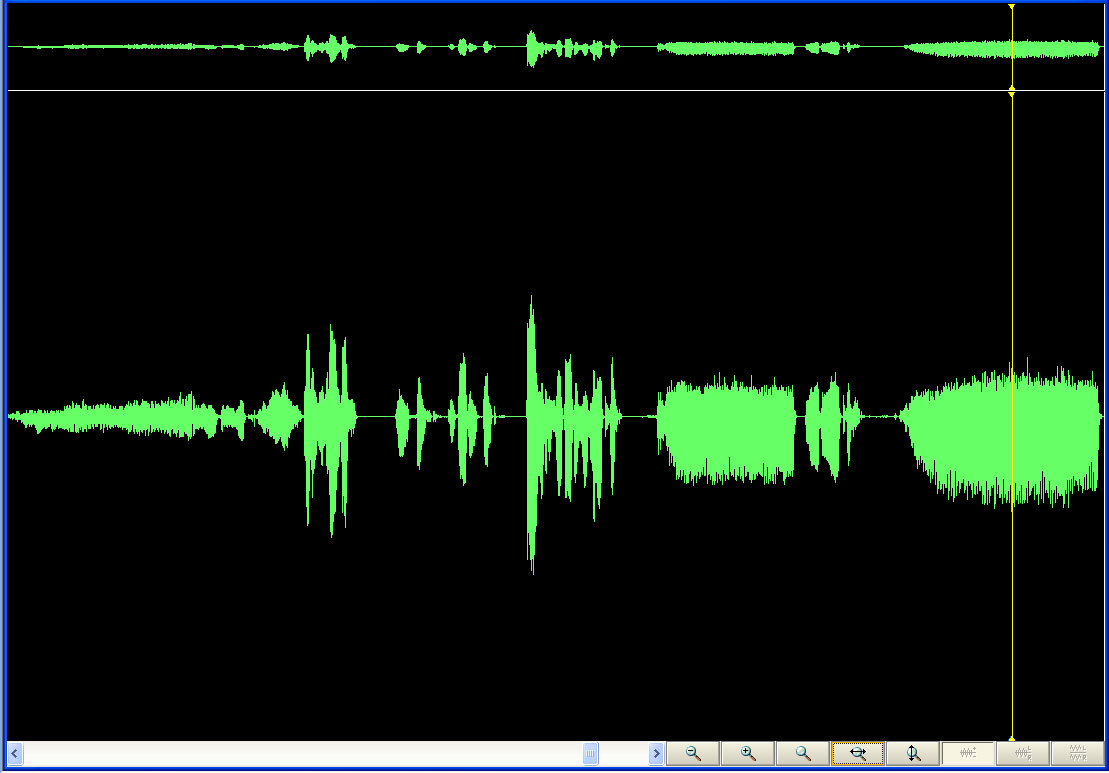
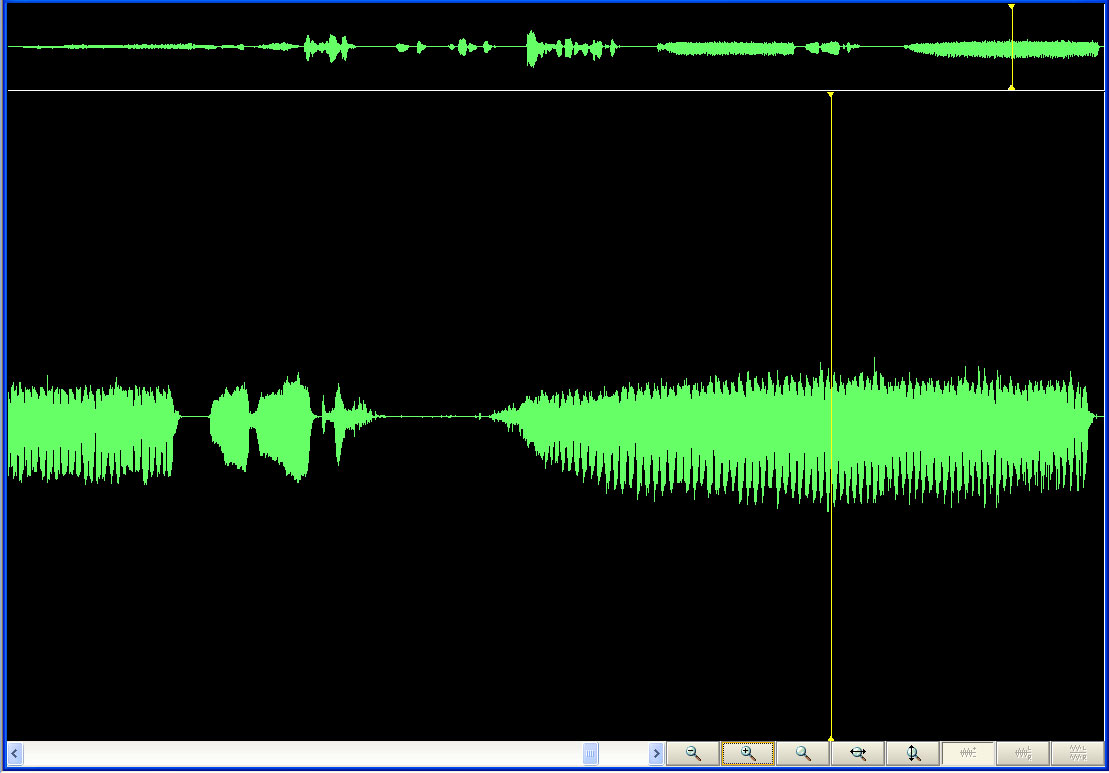
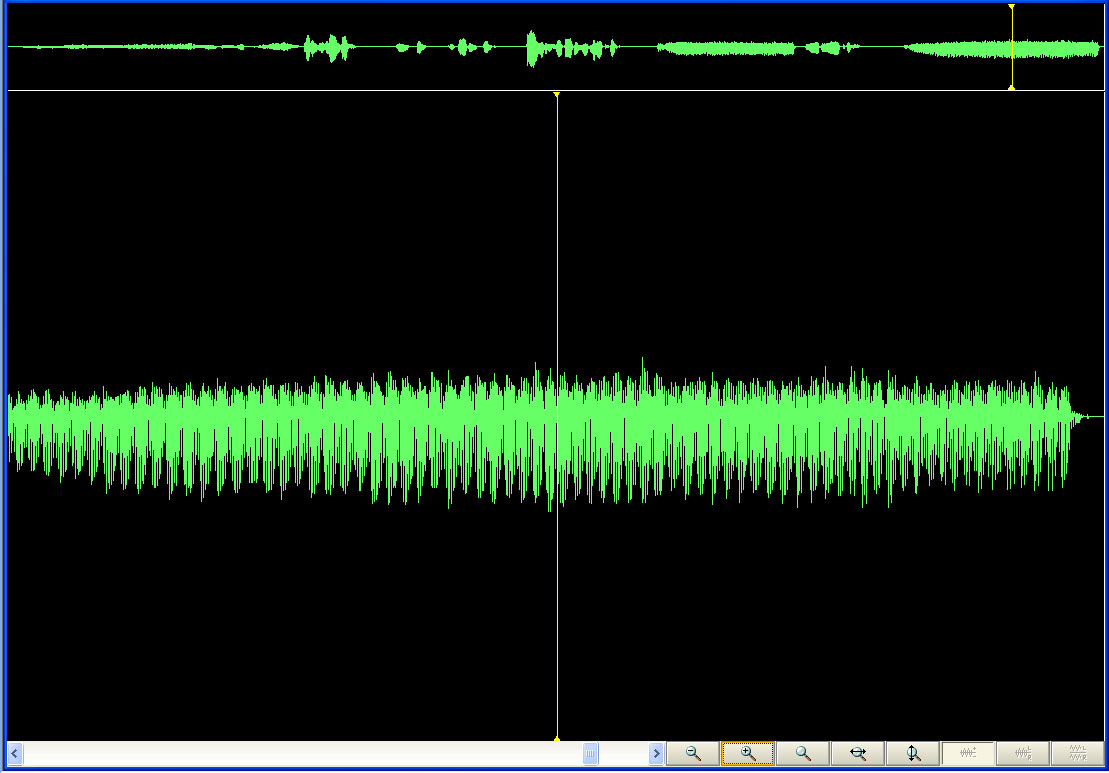
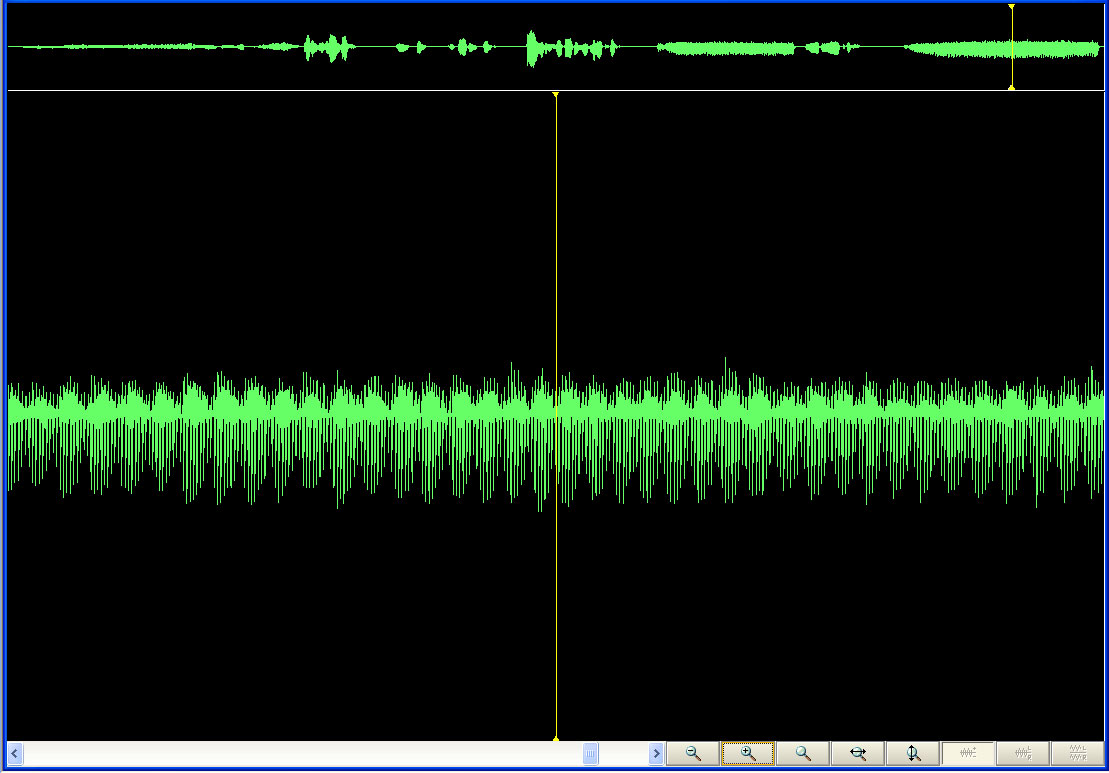
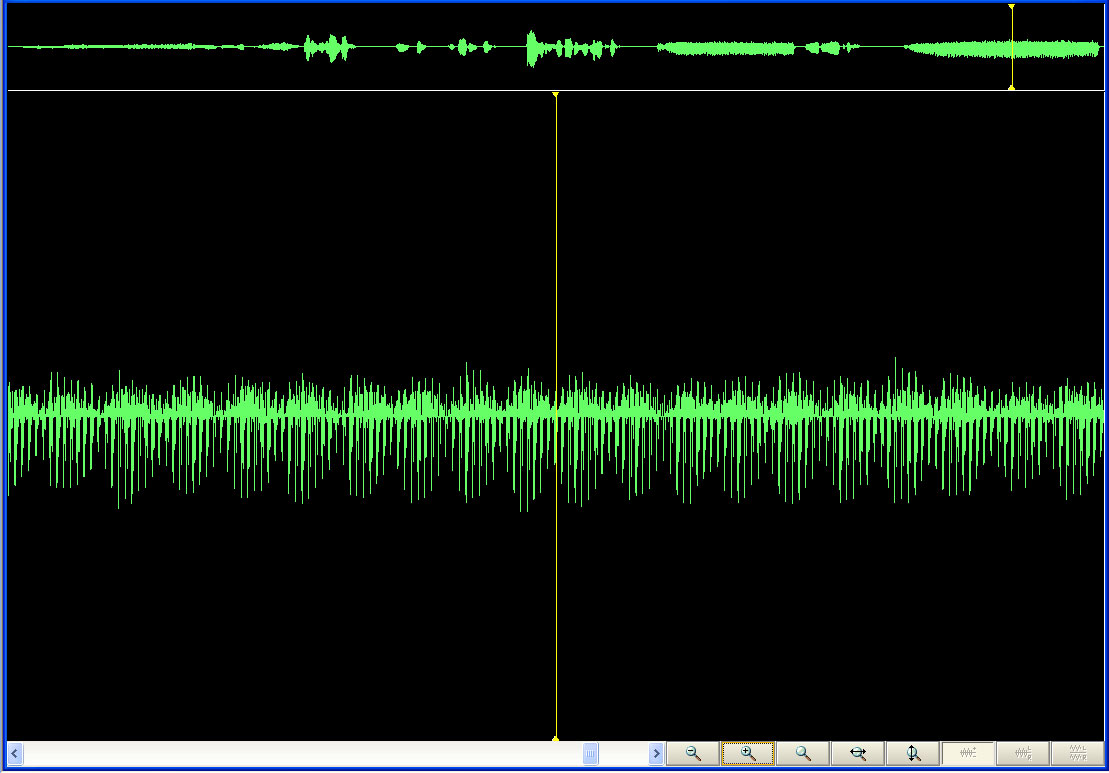
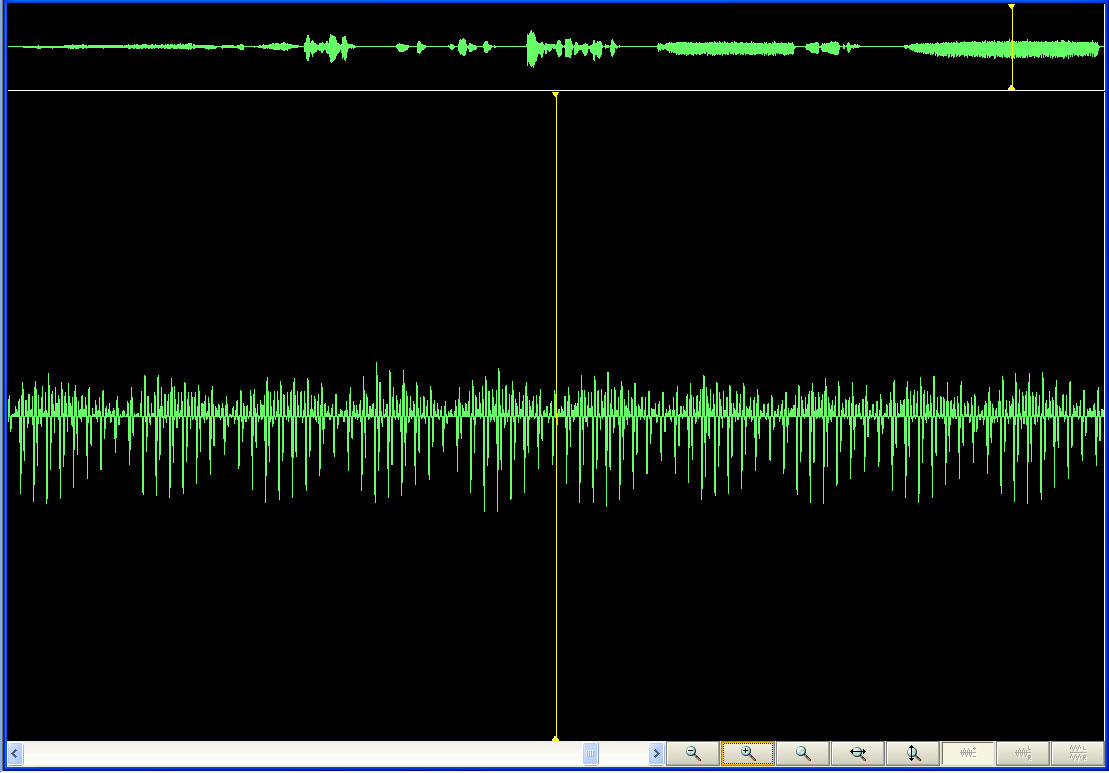
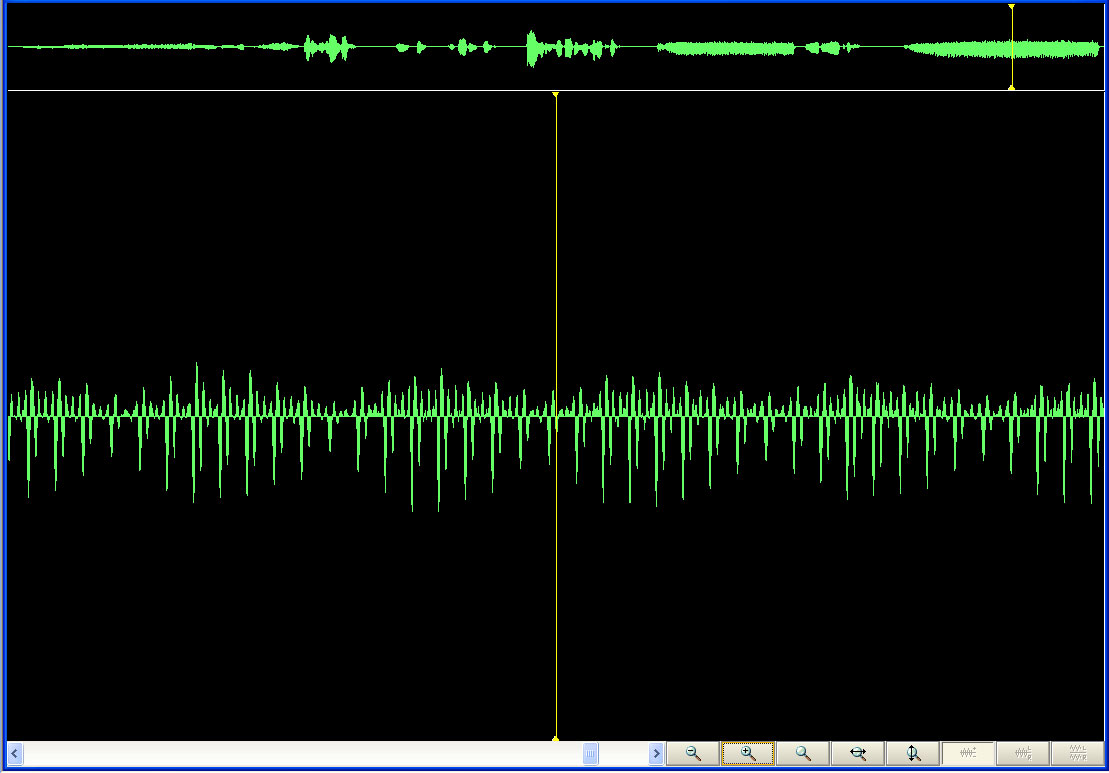
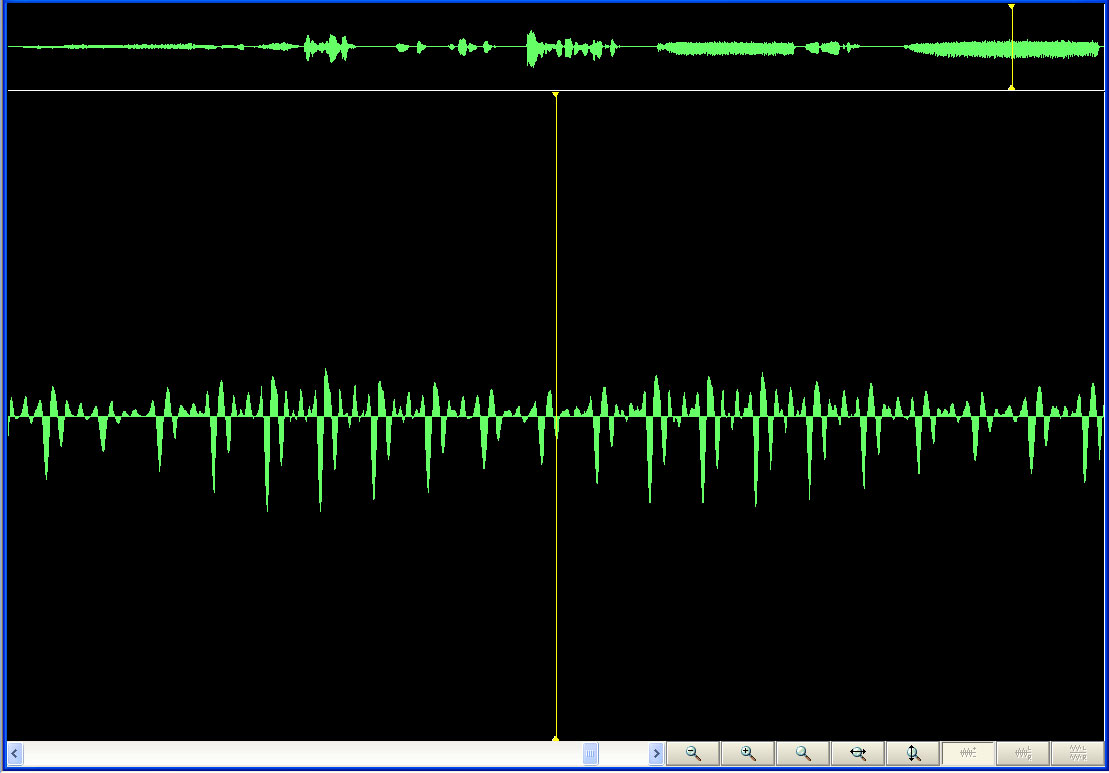
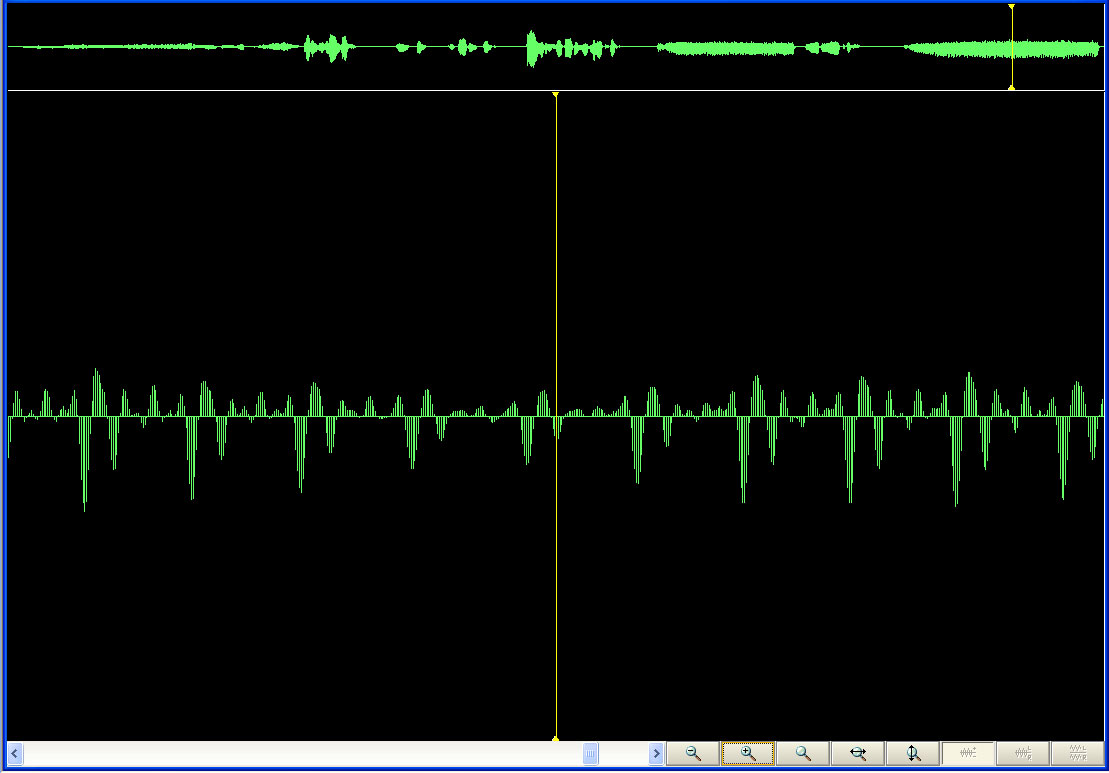
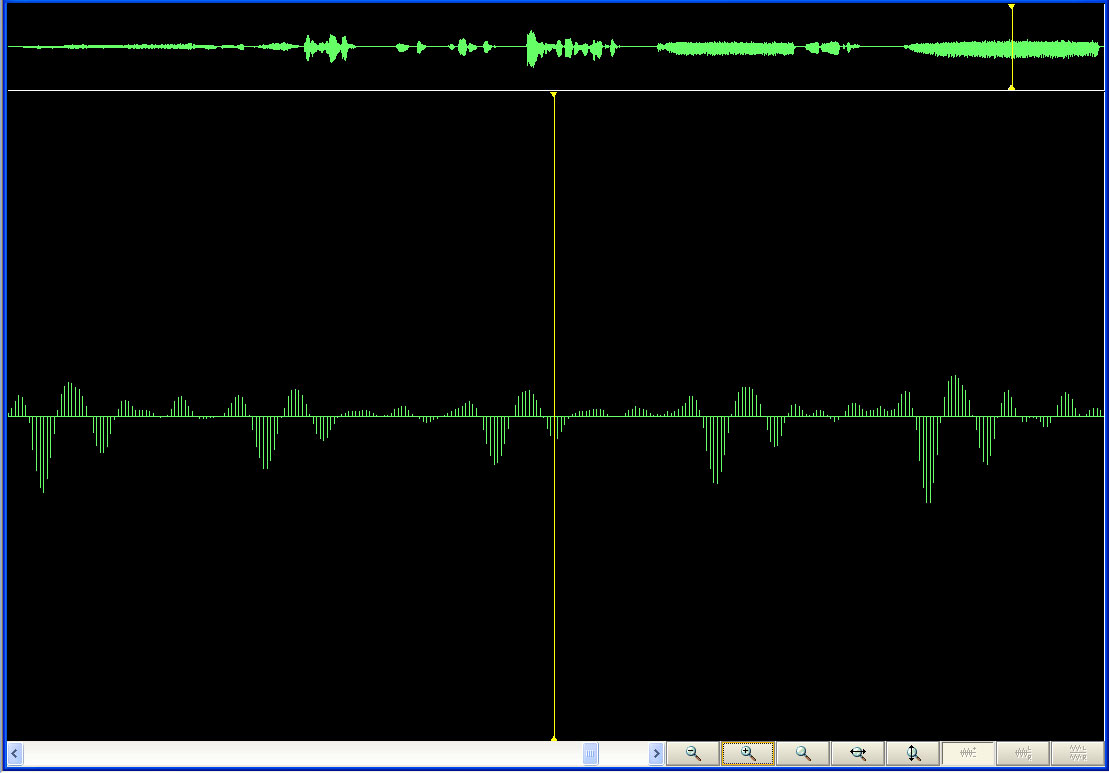
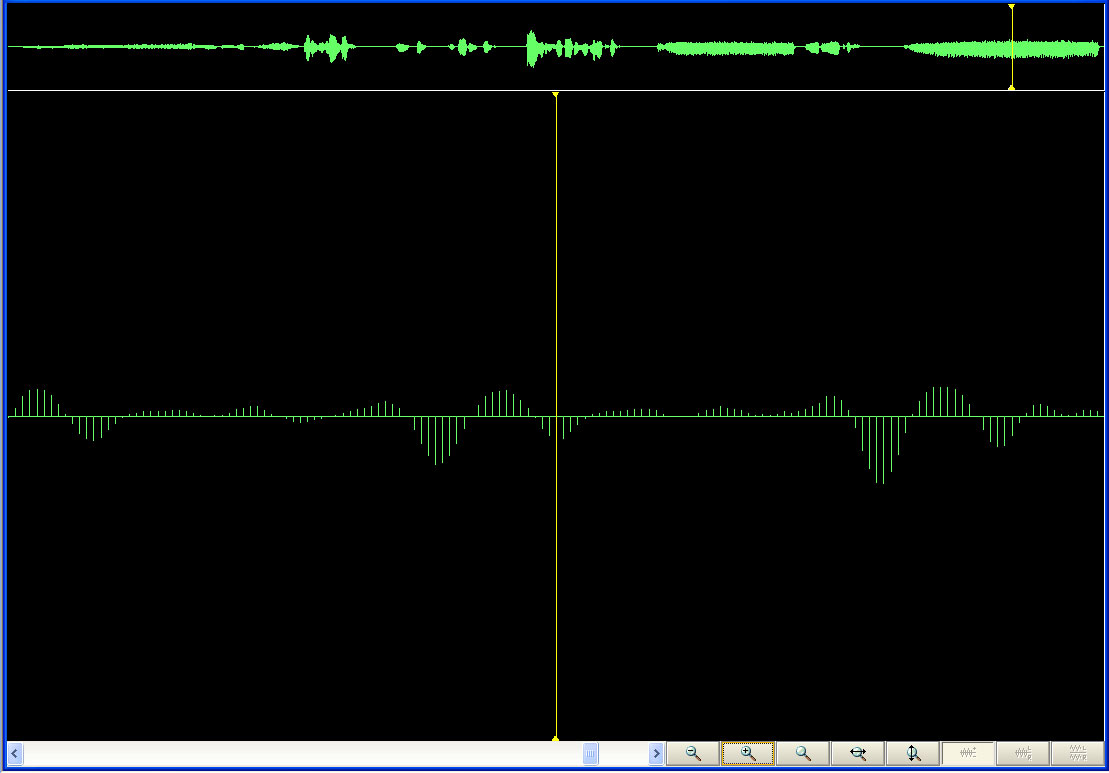
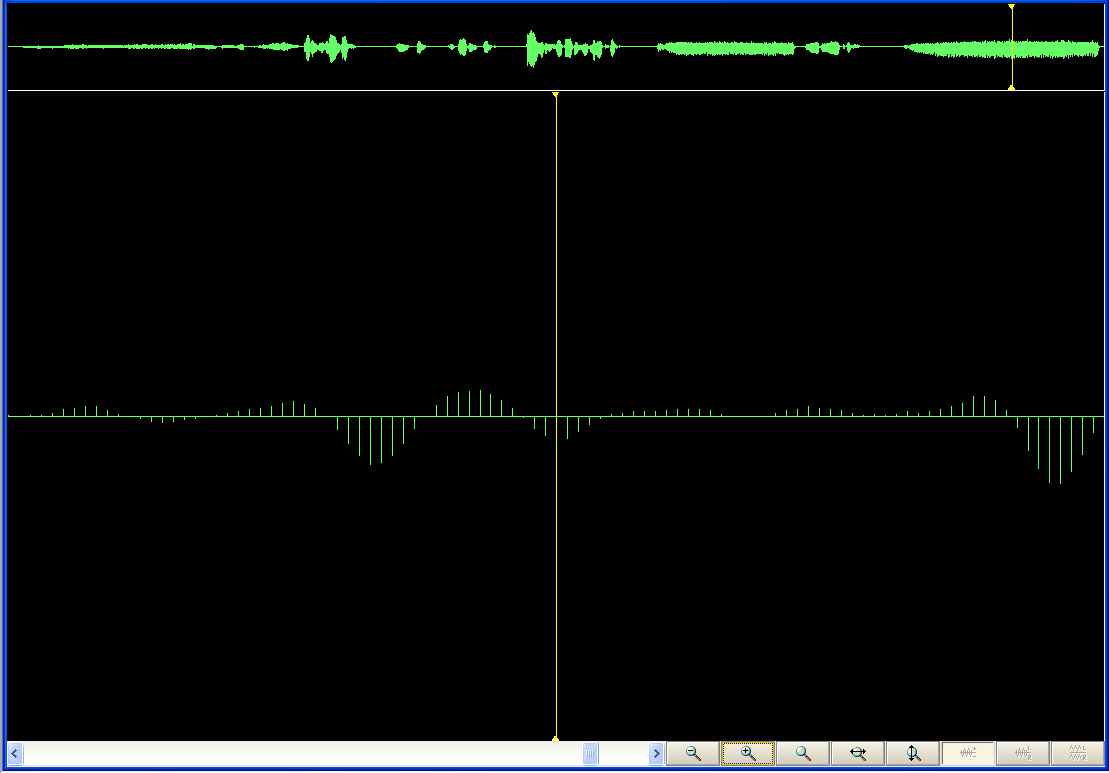
Listen to the sounds of the author making uvular trills in the linked .wav file. Figure 1 shows an
animation of the visual profile of the sounds. Note the
regularity of pattern. The animation first shows the entire
pattern. It then successively zooms in on the yellow line
retained in original position in the strip at the top and altering
position in the screen filling most of the animation.

|
Figure
1. Animation of view of uvular trill sound at successive levels
of detail. Note the periodicity in the final sound (yellow line
centered in it as a reference line).
Figure 2 shows the pattern as a set of 12 screen captures. The
reader wishing to have animation, but also to have control to stop it
at will, might wish instead to view the linked
movie file.
Do individuals who can easily replicate this pattern have a greater or
lesser likelihood of sleep apnea? Is there a relationship at
all? It might be an interesting question to pusue!
References
Wikipedia,
Stalagtite,
http://en.wikipedia.org/wiki/Stalagmite
Wikipedia,
Uvula, http://en.wikipedia.org/wiki/Uvula
Wikipedia,
Uvular Trill, http://en.wikipedia.org/wiki/Uvular_trill
Persistent URL: http://deepblue.lib.umich.edu/handle/2027.42/58219
Software
used:
Adobe Photoshop
WavePad Master's
Edition, NCH Software.
Solstice:
An Electronic Journal of Geography and Mathematics,
Volume
XIX, Number 1
Institute
of Mathematical Geography (IMaGe).
All
rights reserved worldwide, by IMaGe and by the authors.
Please
contact an appropriate party concerning citation of this article: sarhaus@umich.edu
http://www.imagenet.org